Iowa Eye Association News
Oct. 2004. Series 2, no. 39.
Iowa Eye Association News Oct. 2004. Series 2, no. 39. |
Article prepared by
Randy H. Kardon, MD, PhD
After gaining considerable experience with optical coherence tomography (OCT2) since July 2000, The University of Iowa Department of Ophthalmology & Visual Sciences has integrated the newer OCT3 (Stratus) into clinical practice in many areas of diagnosis and management of retinal and optic nerve disorders.
OCT is being used to diagnose and monitor optic nerve disorders by determining the degree of retinal ganglion cell-axonal loss resulting in thinning of the retinal nerve fiber layer. Thinning is monitored most frequently in glaucoma, since there are a number of patients with early glaucoma who have normal visual field, but pathologic thinning of the retinal nerve fiber layer, compared to age-matched normals. In addition, OCT of the retinal nerve fiber layer may be useful in monitoring for any signs of progressive damage and establishing the need for further treatment. The UIHC Ophthalmology Department has also been studying the reproducibility of the measurement on the same day and longitudinally on five different test visits. Some of these patients are enrolled as part of a funded 5-year Veterans Administration Merit Review study by Dr. Michael Wall to study what constitutes the best method for detecting progression of optic nerve damage, especially in glaucoma. These patients are extensively tested for function using different types of perimetry and structure (using OCT and disc photographs) over 4 years. An incredible amount of information will be forthcoming which will help clinicians to determine what constitutes worsening and whether objective measures indicate treatment changes are warranted.
In compressive optic neuropathy, I have received a 3-year VA grant to determine the use of retinal nerve fiber layer analysis in predicting recovery of vision (reversible loss of optic nerve function). So far my co-workers and I have found that patients with normal or near normal nerve fiber layer thickness and profound visual loss have a good chance of recovery after surgery or radiation treatment compared to eyes that have thinning or permanent structural loss. Our group is also combining visual field testing as well as electrophysiologic testing - pattern electroretinogram (PERG) and visual evoked potentials (VEP), which are recorded simultaneously as a sensitive measure of the function of the optic nerve proximal and distal to the compression. We are also applying this approach to other optic neuropathies to understand the sequence of events in visual loss and which component may still be reversible.
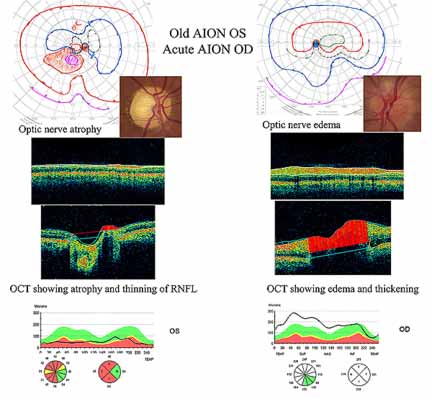
OCT is also being used to follow the course of thickening of the retinal nerve fiber layer due to edema from various causes. Drs. Michael Wall, Andrew Lee, and I are finding that quantification of optic disc edema with OCT may be more accurate and more sensitive than fundus examination of the optic nerve or photos and we are incorporating this into the response to treatment of pseudotumor cerebri and other causes of raised intracranial pressure.
We have also been surprised by a few cases of chronic optic disc edema that revealed vitreous traction on the optic nerve head as the cause of disc edema that was not apparent on fundus examination.
The relationship between structure and function is revealing many aspects of optic nerve damage that were not appreciated before this technology was available. We anticipate further applications in clinical practice as more information becomes available and further improvements in the technology occur.
The University of Iowa Retina Clinic also uses OCT3 extensively to determine subclinical retinal fluid collections in the macula. In some cases, there may not be active leakage on angiography, so OCT is helpful in showing pathologic fluid collection and change over time (worsening or improvement) due to cystoid macular edema, diabetic macular edema, subretinal neovascular membranes, pigmented epithelial detachments, and central serous retinopathy. Sometimes it is very difficult to differentiate fluid from retinal holes, and OCT can be very informative in such cases. One of the most valuable applications is determining the presence or absence of vitreous traction in diagnosing visual loss and planning treatment. Another important application has been the determination of the presence of epiretinal membranes influencing vision.
Although OCT is not a substitute for a detailed biomicroscopic retinal exam, it should be considered a valuable adjunct for qualitative and quantitative assessment of the retina, optic nerve, and vitreous.
image by Dr. Randy Kardon and Susan Anderson
|
(requires Adobe Acrobat Reader) |
|||
| "Together,
we have a vision for the future." |
Copyright © University
of Iowa, 2004 |
||