Case Studies in Ophthalmology
Cases for the Ophthalmology Clerkship
Note to Medical Students on the Ophthalmology Rotation at the University of Iowa:
Print the question and answer sheet (Ctrl-Print or Command-Print) and enter your answers on it. You may prefer to type your answers on this page and then print it. If you do this, be careful that your full answer shows in the printout. Experience with Internet Explorer has been less than optimal.
Return the printed copy with your answers to Michelle Snyder or Dr. Kemp via campus mail (11290 PFP) or scan as a pdf and email to Michelle at michelle-r-snyder@uiowa.edu or Dr. Kemp at pavlina-kemp@uiowa.edu.
Case #50 Nasolacrimal Duct Obstruction
History
Case 1: At about two to four weeks of age, the patient developed “watery” eyes with a tendency for tears to spill over his lower lids unassociated with crying.
Case #1

Case 2: This infant was born with the bluish swelling between the base of the nose and the inner canthus.
Case #2

Enter Full Name (required):
Your email address (required):
Question #1
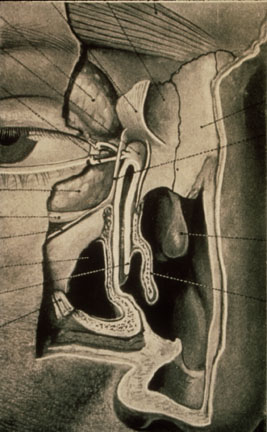
Discuss the anatomy and physiology of the lacrimal drainage system depicted in the following slide.
Photo #3
Question #2
Discuss the causes and natural history of congenital nasolacrimal duct obstruction.
Question #3
Discuss the treatment options of nasolacrimal duct obstruction.
Question #4
What are the potential complications of no treatment?
Question #5
What is the lesion in the second clinical picture (Photo 2) and how does it relate to nasolacrimal duct obstruction?
Question #6
Discuss other causes of tearing in infants and children such as in Photo 1.
References
Kushner BJ: Congenital nasolacrimal system obstruction. Arch Ophthalmol 1982: 100:597-600.
Harris GJ, DiClementi D: Congenital dacryocystocele. Arch Ophthalmol 1982; 100:1763-1765.
Duane T: Biomedical Foundations of Ophthalmology. Harper & Row, pp14-20.
Petersen RA, Robb RM: The Natural course of congenital obstruction of the nasolacrimal duct. J Ped Ophthal 1978; 15:246-250.