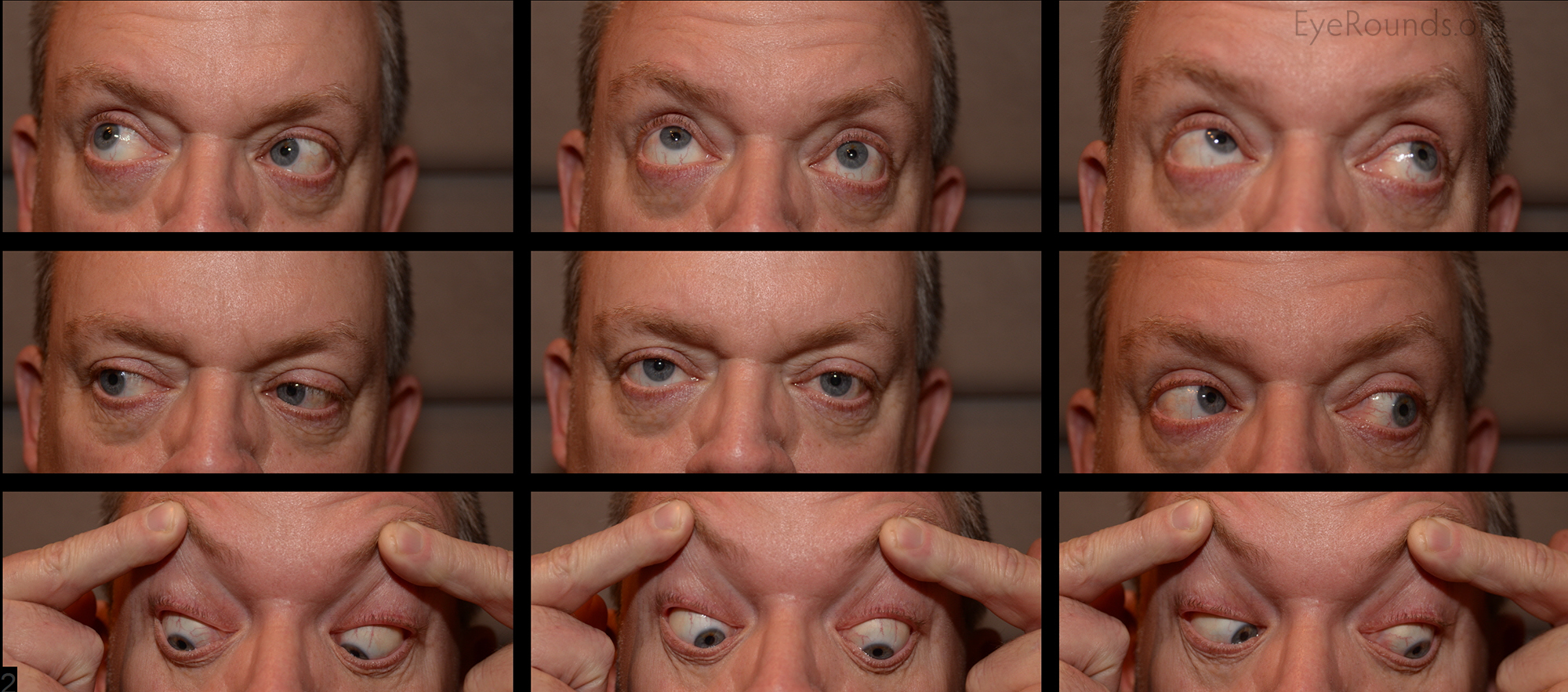
This patient presented after closed head trauma with a complaint of predominantly vertical, binocular diplopia ever since the event. The diplopia was worse with left gaze and improved with left head tilt. He adopted a mild left head tilt and had a right hypertropia in primary gaze. The right hypertropia worsened with left gaze and right head tilt (not pictured). There is underaction of the right superior oblique and overaction of the right inferior oblique that are best appreciated with the right eye in adduction looking in the vertical directions. There was 10 degrees of excyclotorsion on double Maddox rod testing. MRI scan was normal. This presentation was consistent with a traumatic right cranial nerve IV palsy.
Cranial nerve IV (trochlear nerve) innervates the superior oblique muscle which is responsible for depression and intorsion of the eye. Superior oblique weakness will produce binocular vertical or torsional diplopia that is variable with different gaze directions (many times worse with downgaze). Patients will have a hypertropia of one eye relative to the other and may adopt a compensatory head tilt. The Parks-Bielschowsky three-step test will show a hypertropia of the ipsilateral eye that worsens with adduction and ipsilateral head tilt. Extorsion of the affected eye may be observed on fundoscopic examination or quantified with double Maddox rod testing.p>

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links