Common feature of fungal keratitis classically include dry-appearing, elevated infiltrates with feathered margins and satellite lesions.
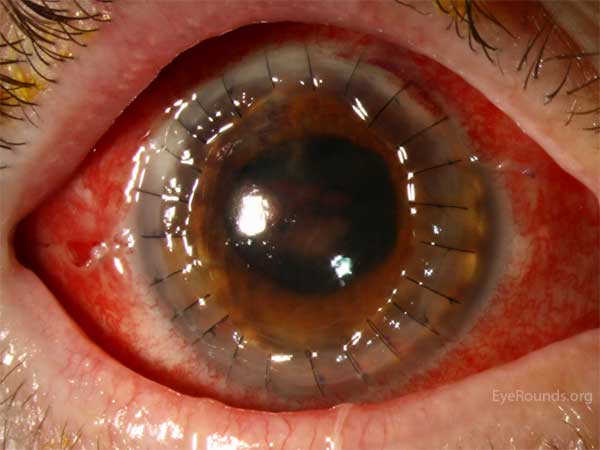
Rapid progression of culture-positive, fulminant Fusarium keratitis over the course of one week. Note the feathered edges, satellite lesions, and large hypopyon. This case required urgent, therapeutic penetrating keratoplasty with anterior chamber washout using amphotericin B and voriconazole to clear the infection.
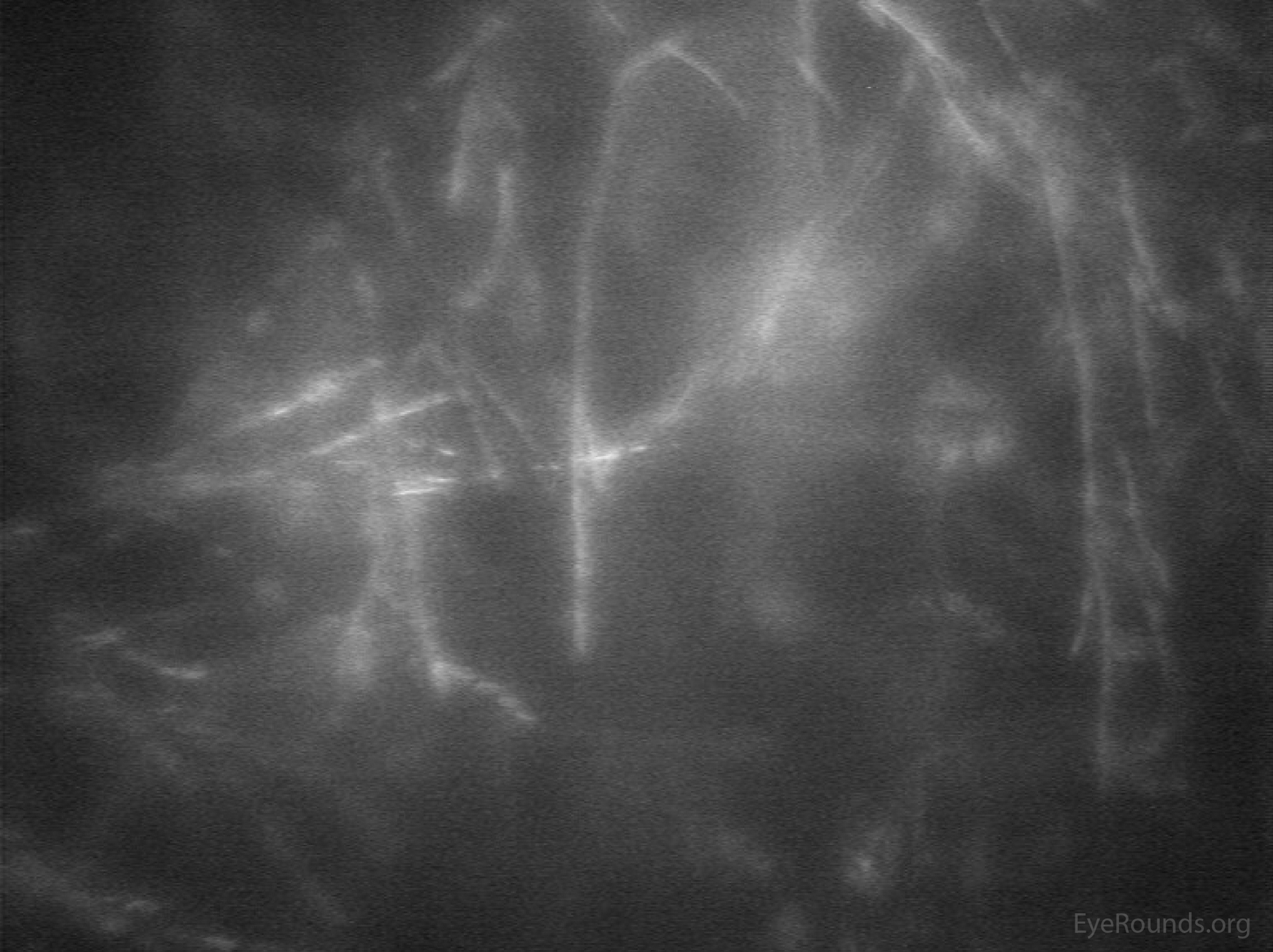
Confocal microscopy showing branching Fusarium filaments in vivo, obtained from the patient in Figure 1 upon her initial presentation.
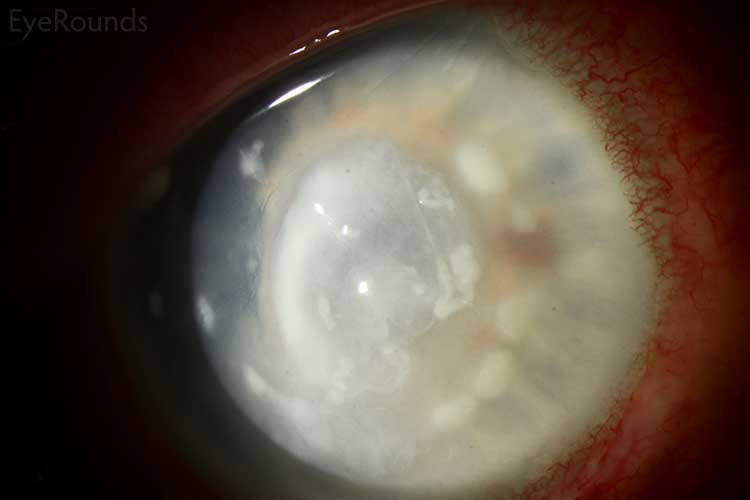
Another patient with severe Fusarium keratitis, showing a late suppurative appearance mimicking bacterial keratitis. This patient eventually developed intraocular extension and endophthalmitis.
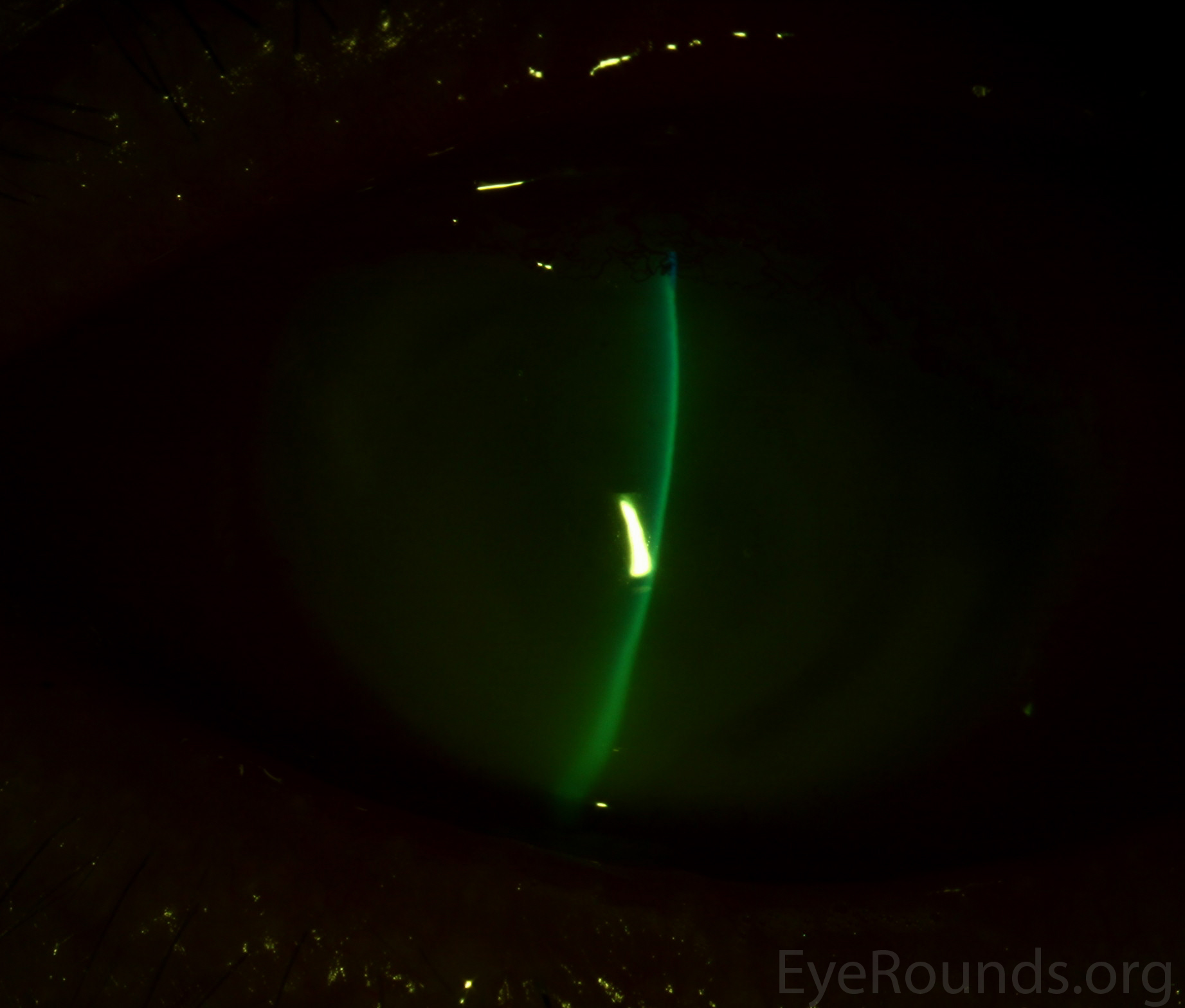
43-year-old male with fungal keratitis from Aspergillus. Note the feathery edges of the infiltrate and the elevated appearance of the lesion, which are commonly seen in fungal keratitis. There is also a 1 mm layered hypopyon

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links