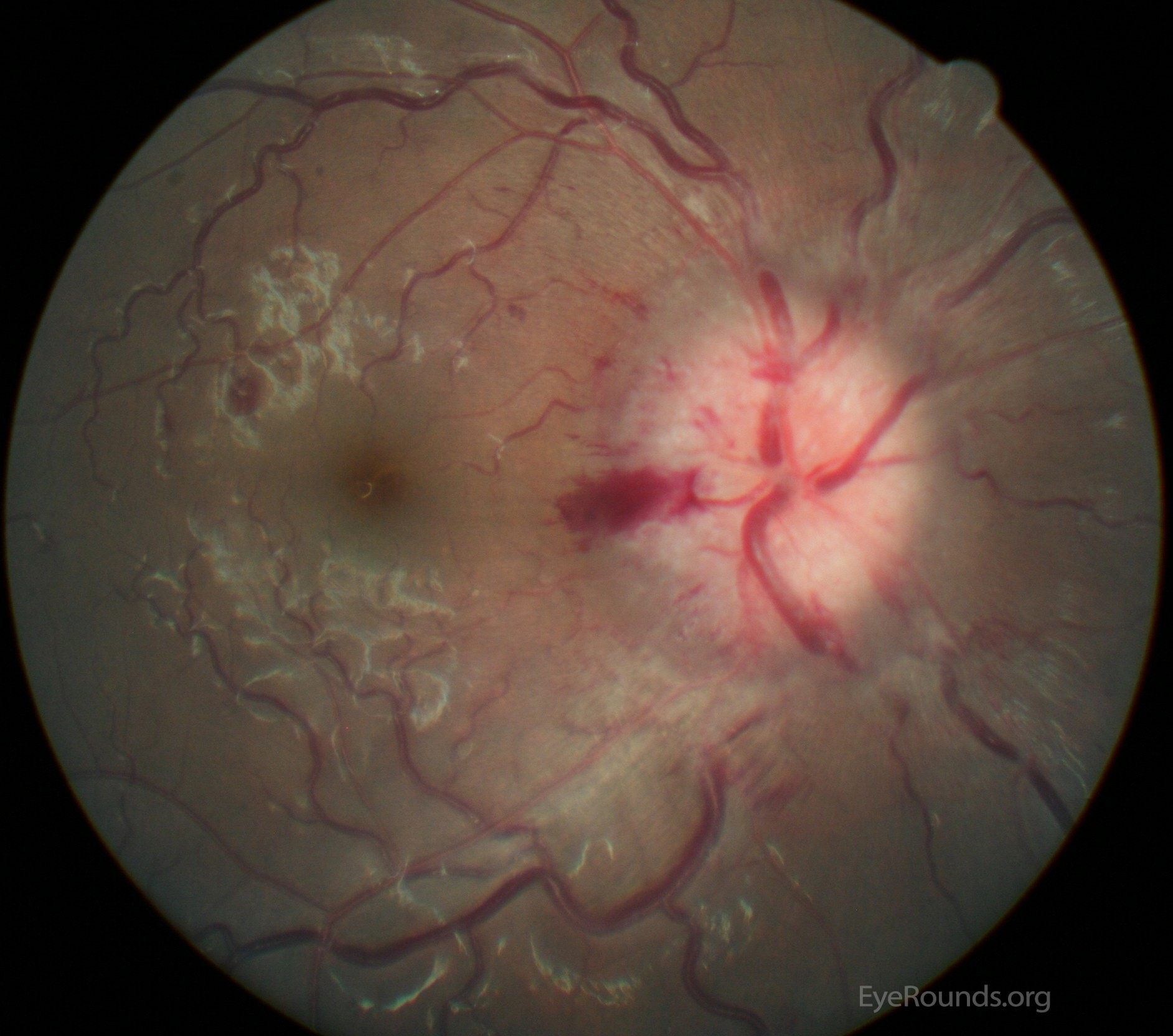
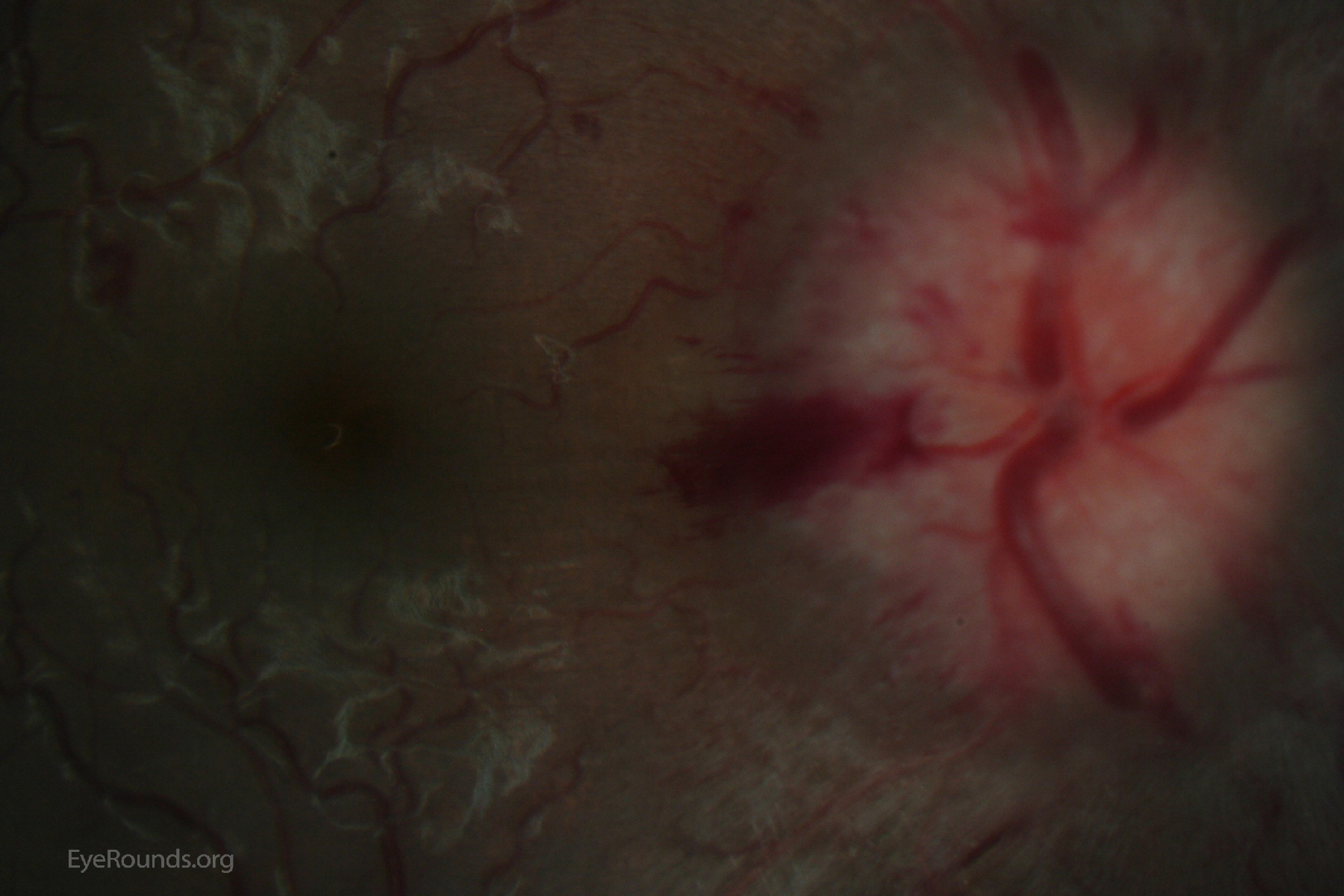
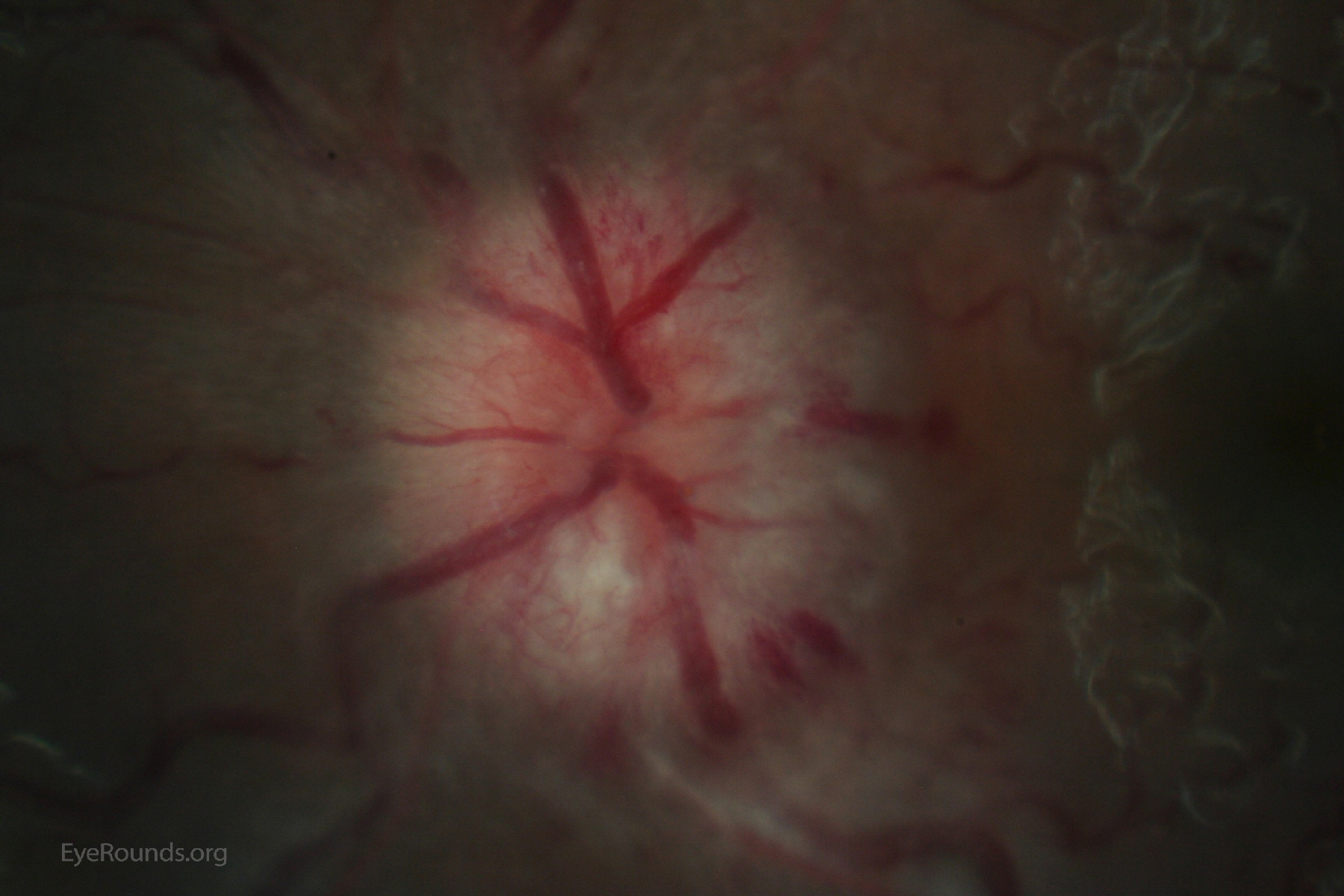
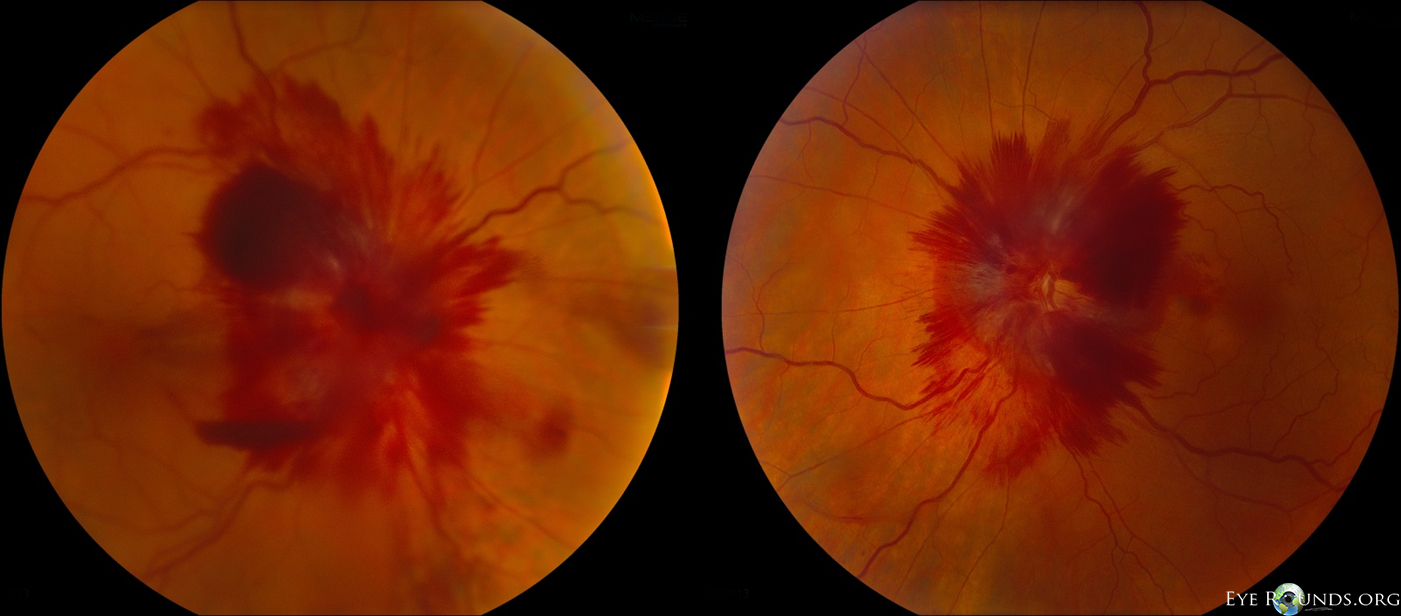
Increased intracranial pressure can have multiple ocular manifestations. Since the optic nerve is wrapped in the meninges, increased pressure in the cerebrospinal fluid (CSF) space can result in forward displacement and edema of the optic nerves. Bilateral disc edema should always carry a high suspicion of papilledema.
Papilledema is potentially sight threatening and many of the conditions that produce it are life threatening. Hemorrhages on the optic disc are associated with acute rather than long-standing edema.
A second ocular sign (this patient's presenting complaint but not shown here) of increased intracranial pressure is sixth nerve palsy. Cranial nerve six has a long path from the pons through the prepontine cistern where it ascends the along the clivus. The nerve is tightly tethered to the meninges at Dorello's canal where it pierces through the clivus to enter the cavernous sinus. A rise in intracranial pressure can stretch cranial nerve six in this location resulting in a nerve palsy. While isolated, unilateral cranial nerve six palsy is more likely to be vascular in origin, bilateral cranial nerve six palsy is highly suspicious for increased intracranial pressure.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links