Chief Complaint: Night-blindness
History of Present Illness: A 55-year-old male presented with a complaint of gradual onset, progressive night blindness over the past six months. He had given up driving because he could not see the lane markers on the road. All forms of artificial light seemed dim; however, daytime vision seemed perfectly normal. Prior to the onset of these symptoms, he had never had any ocular problems. He had no difficulty distinguishing colors.
Past Ocular History: None
Medical History: The patient suffered from a mesenteric vein thrombosis 4 years prior to presentation. He underwent surgical resection of about 3 feet of his small intestine, ascending, and transverse colon. During the resection, he was found to have a cirrhotic-appearing liver. An extensive work-up was consistent with non-alcoholic steatohepatitis. He had chronic anemia as well as chronic fatigue.
Medications: Spironolactone, furosemide, multivitamin
Allergies: No known drug allergies
Family History: No retinitis pigmentosa
Social History: The patient does not smoke or drink.
|
|
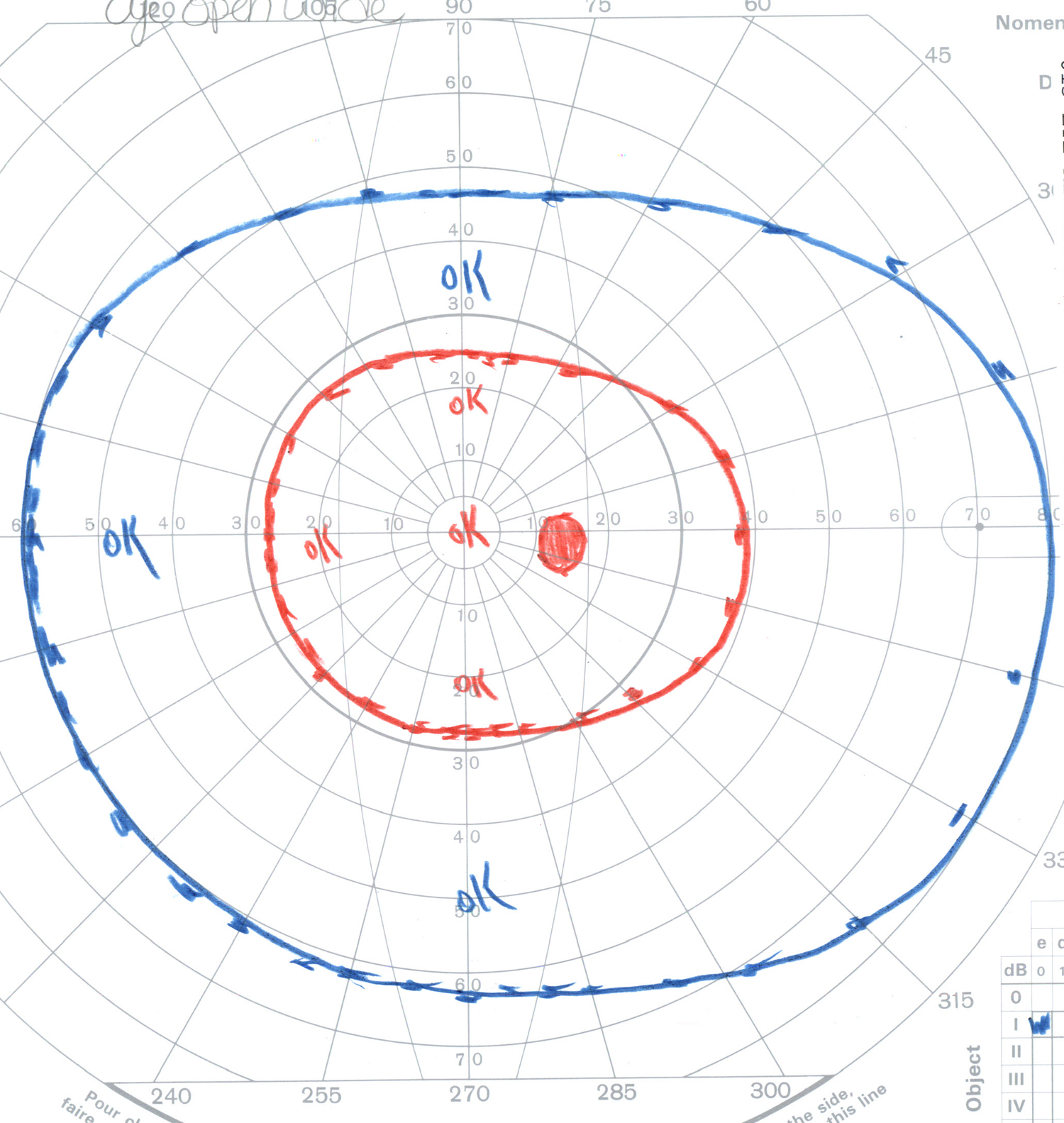
A Goldmann visual field revealed mild constriction of the I2e isopter in the left eye. The right eye had a nearly normal visual field (Figure 2).
|
|
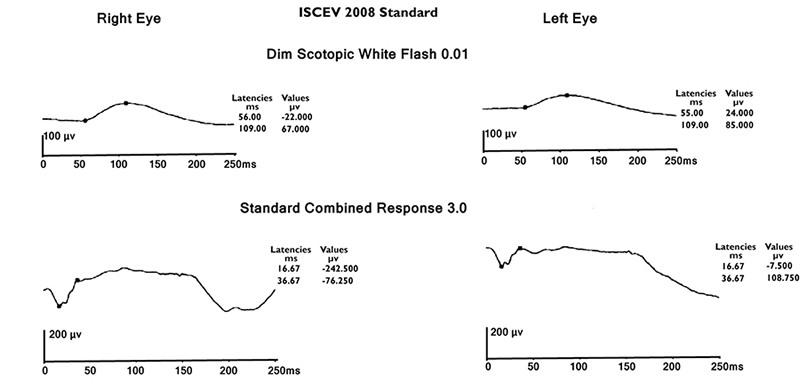
The patient underwent electroretinography (ERG). The scotopic bright flash, or maximal combined response, was decreased in both eyes with a value of 165 microvolts OD and 95 microvolts OS (normal range is >255.4 microvolts). The scotopic dim flash, or rod response, was decreased in the left eye with a value of 60 microvolts (normal range is >72.42 microvolts). The implicit times, photopic bright response, and 30 Hz flicker were all normal.
|
These findings suggested an acquired form of rod photoreceptor disease leading to night-blindness. In the setting of bowel resection, vitamin A deficiency was considered as a possible etiology; therefore, a vitamin A level was drawn. Vitamin A levels normally range between 0.30-1.20 mg/L, but the patient's vitamin A level measured only 0.12 mg/L. He was started on oral vitamin A 10,000 international units (IU), twice a day.
After one month of treatment, the patient reported that his vision had returned to normal, and he had started driving at night again without any problems. His visual acuity had improved to 20/15 OU. His vitamin A level was still below normal but had increased to 0.18 mg/L. A repeat Goldmann visual field was performed at that visit which showed an improvement in both visual fields (Figure 4).
|
|
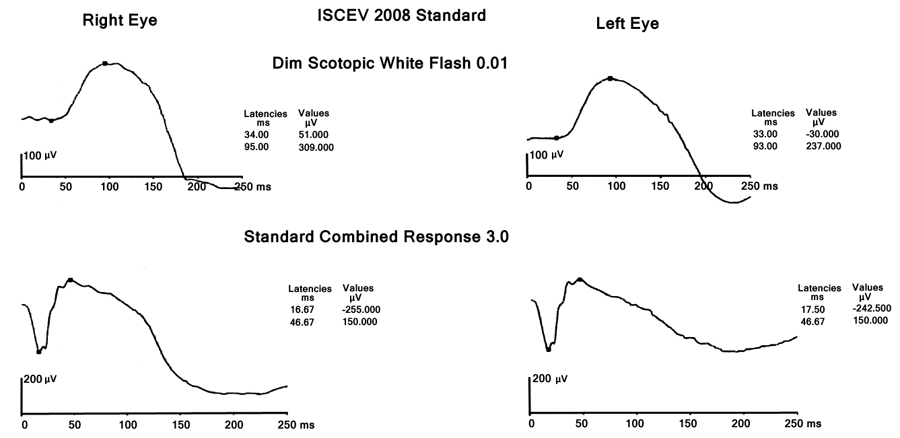
Two months after starting treatment, an ERG was repeated which revealed a complete resolution of the rod photoreceptor disease. The maximal combined response was 445 milivolts OD and 395 millivolts OS (normal value is >253.8) (Figure 5).
|
Vitamin A deficiency is the leading cause of childhood blindness in the developing world. In the United States, vitamin A deficiency can occur as a result of malnutrition, malabsorption, or poor vitamin metabolism due to liver disease (Braunstein et al 2010, Chae and Foroozan 2006, Smith and Steinemann 2000). Malabsorption of vitamin A has been documented to occur after bariatric surgery (Lee et al 2005).
Xerophthalmia is a term used to describe the spectrum of ocular disease that can arise from vitamin A deficiency. These changes include dry eye (xerosis), corneal ulceration and melting (kerotomalacia), night blindness (nyctalopia), and retinopathy. Vitamin A is also essential for immune function, and affected children are more susceptible to severe infections, such as measles (Smith and Steinemann 2000).
Vitamin A is ingested in the form of retinaldehyde from milk, meat, fish, liver, and eggs. It is also ingested as carotene from green leafy vegetables, yellow fruits, and red palm oil. These compounds are stored in the liver in the form of retinyl pamitate. The aldehyde form of vitamin A, retinal or retinaldehyde, combines with the protein opsin in the rods to create rhodopsin, which is a photosensitive pigment. A similar process takes place in the cones. During phototransduction, some retinal is lost so a constant supply of vitamin A is needed. Vitamin A deficiency can therefore lead to night blindness with associated visual field changes and a depressed ERG (Smith and Steinemann 2000, Genead et al 2009). Vitamin A is also necessary for the maintenance of specialized epithelial surfaces. In the conjunctiva, loss of goblet cells and squamous cell metaplasia leads to dryness or xerosis. Bitot's spots are perilimbal gray plaques of keratinized conjunctival debris overlying an area of xerosis (Smith and Steinemann 2000, Sommer 1990). A full-thickness liquefactive necrosis of the cornea (keratomalacia) can also occur. Lee et al 2005). Finally, retinopathy in the form of yellow or white punctuate dots can be seen in the retinal periphery (Genead et al 2009).
Testing for vitamin A deficiency is available in the form of retinol, retinyl pamitate, and retinol binding protein levels. The World Health Organization recommends 200,000 IU of vitamin A for 2 days followed by another dose 2 weeks later for severely malnourished children older than 12 years of age with vitamin A deficiency (WHO 1999); however, more recent case studies have shown that much less supplementation can lead to reversal of symptoms (Chae and Foroozan 2006). Vitamin A can also be given intramuscularly if there is a concern for severe malabsorption or corneal involvement requiring a faster recovery.
Our patient had a fairly quick recovery on oral vitamin A supplementation with 10,000 IU twice a day. This case illustrates the importance of considering vitamin supplementation in all patients who have undergone bowel resection, especially in patients with underlying liver disease.
Diagnosis: Vitamin A deficiency due to malabsorption
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Privett B, Mahajan VB. Vitamin A Deficiency and Nyctalopia: 55-year-old male with gradual onset of night blindness. EyeRounds.org. February 22, 2011; Available from: https://eyerounds.org/cases/130-vitamin-a-deficiency.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links