
Chief Complaint: Painless central vision loss in the left eye
History of Present Illness: This adult female presented to the comprehensive ophthalmology clinic with painless central vision loss in the left eye, recently detected on an employee screening examination. She had noted difficulty with reading and an opaque “white light” in her central vision of the left eye.
Past Ocular History: Negative for surgery or trauma
Past Medical History: Hypothyroidism
Medications: Levothyroxine
Family History: Negative for cancer or ocular disease
Social History: Machinist, longtime smoker
Review of Systems: Negative, including no weight change, mood change, fatigue, or loss of libido.
Visual acuity without correction: 20/25 right eye (OD), 20/125 with eccentric fixation left eye (OS)
Intraocular pressure: 10 mmHg OD, 12 mmHg OS
Pupils: 5 → 3 mm in both eyes (OU), brisk reaction OU, 0.3 log-unit relative afferent pupillary defect OS
Confrontation visual fields: temporal loss OD, central scotoma OS
Anterior segment: 1+ nuclear sclerosis OU, otherwise normal
Fundus: Temporal optic nerve pallor OU; normal macula, vessels, and periphery OU (Figure 1)
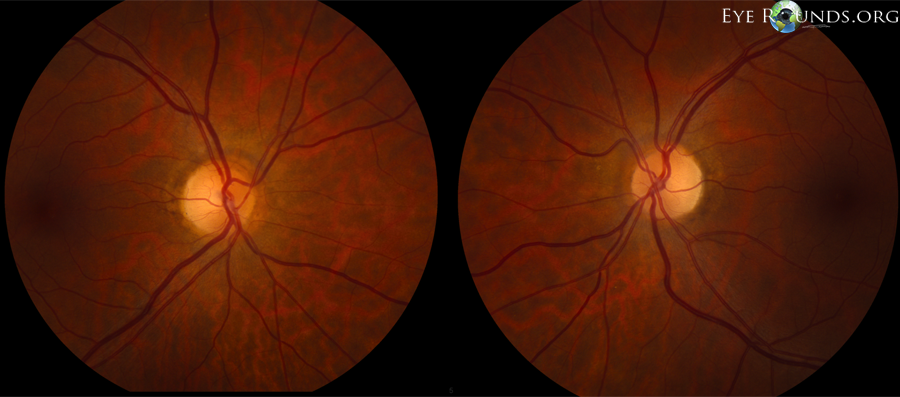
Figure 1: Color fundus photographs, revealing temporal optic nerve pallor OU. (click image for higher resolution)

Figure 2: Significant temporal field loss respecting the vertical meridian OD, cecocentral scotoma with inferotemporal field loss largely respecting the vertical meridian OS. (click image for higher resolution)
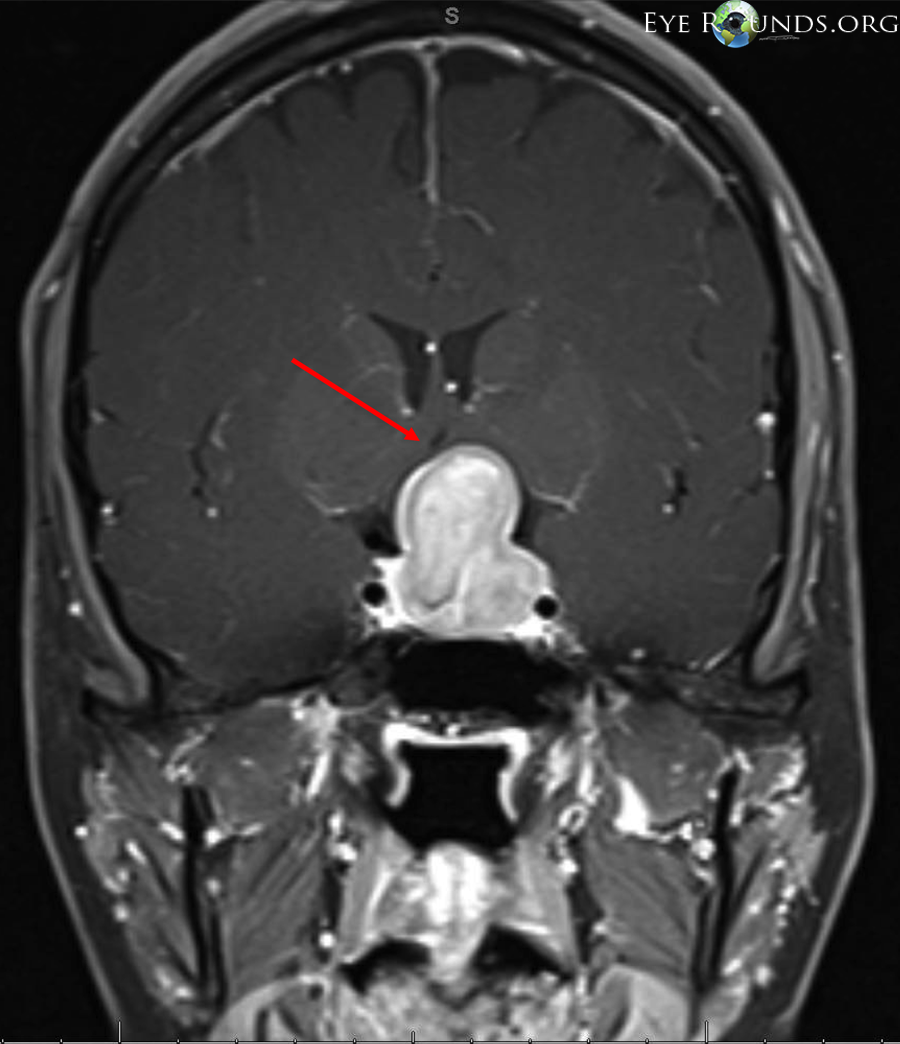
Because of her decreased visual acuity, bitemporal visual field loss, and temporal optic nerve pallor OU, there was concern for intracranial pathology affecting the optic chiasm, and the patient was referred to neuro-ophthalmology. Contrast-enhanced magnetic resonance imaging (MRI) of the patient’s brain was ordered (Figures 3-4).
 |
 |
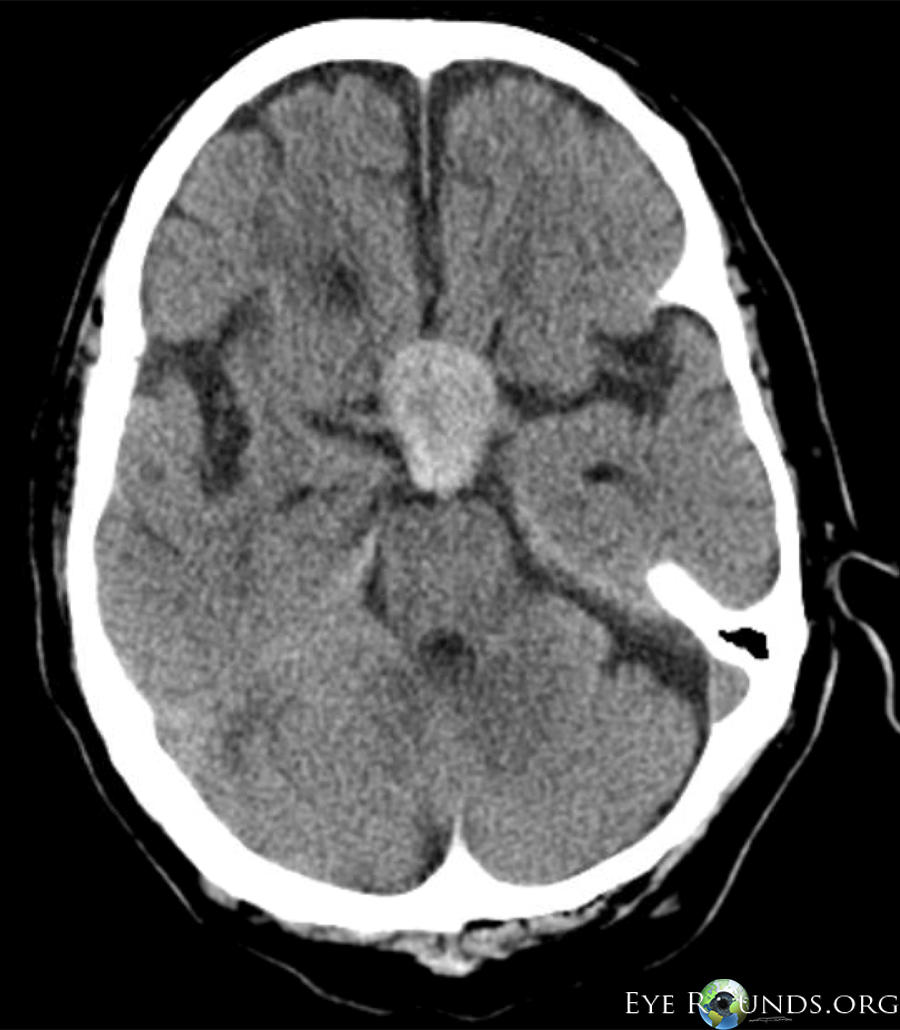
| Figure 3: Post-contrast T1 brain MRI, coronal view, showing a pituitary adenoma with elevation and compression of the optic chiasm (arrow indicates area of optic chiasm) | Figure 4: Post-contrast T1 brain MRI, axial view, showing a pituitary adenoma with compression of the optic chiasm (sagittal view unavailable) |
After the MRI revealed the sellar/suprasellar mass, the patient was referred to neurosurgery. Endocrine laboratory testing was used to determine if this tumor was a lactotrophic adenoma (“prolactinoma”), because such tumors are typically treated medically with dopamine agonist therapy (e.g. bromocriptine, cabergoline) as an adjunct to, or in some cases, a substitute for surgery. The patient’s hormone levels indicated that this was not a lactotrophic adenoma, and shortly thereafter she underwent transsphenoidal gross total resection of the tumor with placement of a space-filling fat graft. At the time of publication, she had yet to follow up in the neuro-ophthalmology clinic for postoperative evaluation.
Vision loss is a relatively common presenting complaint in a comprehensive ophthalmology clinic. One technique that helped provide effective care in this case was using a 90-diopter lens at the slit lamp to assess the patient’s optic nerves prior to pupillary dilation. Doing so, and noting bilateral temporal pallor of the optic nerves, emphasized the need for visual field testing, which would not have been as accurate had this finding been discovered after dilation.
The results of this patient’s kinetic perimetry testing, showing bitemporal field loss respecting the vertical meridian with a cecocentral scotoma in one eye, were consistent with a junctional scotoma, which indicates a lesion at the junction of the optic chiasm and one optic nerve. Specifically, in this patient the left optic nerve and the optic chiasm were most affected, as evidenced by the visual acuity loss OS and the temporal visual field loss OD with preservation of visual acuity. Thus, our chief concern was for a sellar mass. It is important to note that while a sellar mass may present with bitemporal hemianopia, the combination of findings described above describing a junctional scotoma also localizes to the sellar area, and additional workup is indicated. It is also useful to note that while the classic presentation of junctional scotoma includes central visual field loss in one eye and superotemporal field loss in the contralateral eye, the vision loss in the contralateral eye need not be supertemporal, and was not in this case. Bitemporal hemianopia and junctional scotomas are both findings that may be present in the “chiasmal syndrome,” which describes visual field defects from compression of the optic chiasm.
A few radiologic clues can help differentiate between the various types of sellar masses. Craniopharyngioma is notable for its heterogenous radiographic appearance, often containing cysts and calcifications, which are best viewed on computed tomography (CT). The pituitary adenoma typically lacks these features, though heterogeneity may be present if hemorrhage has occurred. Because of their soft texture, these tumors are usually compressed at the diaphragma sella, resulting in a characteristic “snowman” appearance on coronal sections on MRI, as seen above in Figure 3 [1]. A parasellar meningioma is a potential mimic of the pituitary adenoma, but has a comparatively harder texture, preventing it from compressing at the diaphragma sella, and therefore no “snowman” appearance.
Pituitary adenoma is the most common cause of the chiasmal syndrome [2], and may present at any age. The tumor is classified based on size as either a microadenoma (<10 mm) or a macroadenoma (>10 mm). The pituitary gland produces a variety of hormones, and as such a pituitary tumor may be secretory or nonsecretory. Classically, the nonsecretory tumor presents with vision loss, whereas patients with secretory tumors are usually referred to ophthalmologists for evaluation after having already been diagnosed because of endocrine derangements.
The dreaded complication of pituitary adenoma, and one with which the ophthalmologist must be familiar, is pituitary apoplexy. This life-threatening complication results from acute hemorrhage or infarction of the tumor. Reported incidence varies between 0.6% and 10% of all pituitary adenomas [3]. Although trauma, blood pressure changes, and pregnancy can be predisposing factors, most cases occur spontaneously [4]. Presenting systemic features include severe headache, nausea, and altered mental status. Visual symptoms and signs include vision loss, diplopia, and multiple cranial nerve palsies secondary to rapid expansion of the tumor into the adjacent cavernous sinuses, with cranial nerve III the most commonly affected. Subarachnoid expansion of blood may lead to vasospasm and stroke. Acute endocrine abnormalities, including adrenal crisis and accompanying severe hypotension, can be fatal if not recognized and treated. Treatment is emergent and includes corticosteroids, surgical resection, and supportive measures.
Radiographic findings in pituitary apoplexy may include hyperdensity of the adenoma on CT (Figure 5), combined with relatively mild, patchy contrast enhancement of the tumor on MRI (Figure 6). This is due to hemorrhage-induced expansion and necrosis of the tumor, leading to non-perfusion. Layering hemorrhage in the lateral ventricles can also be seen (Figure 7), which can result in a communicating hydrocephalus.
 |
 |
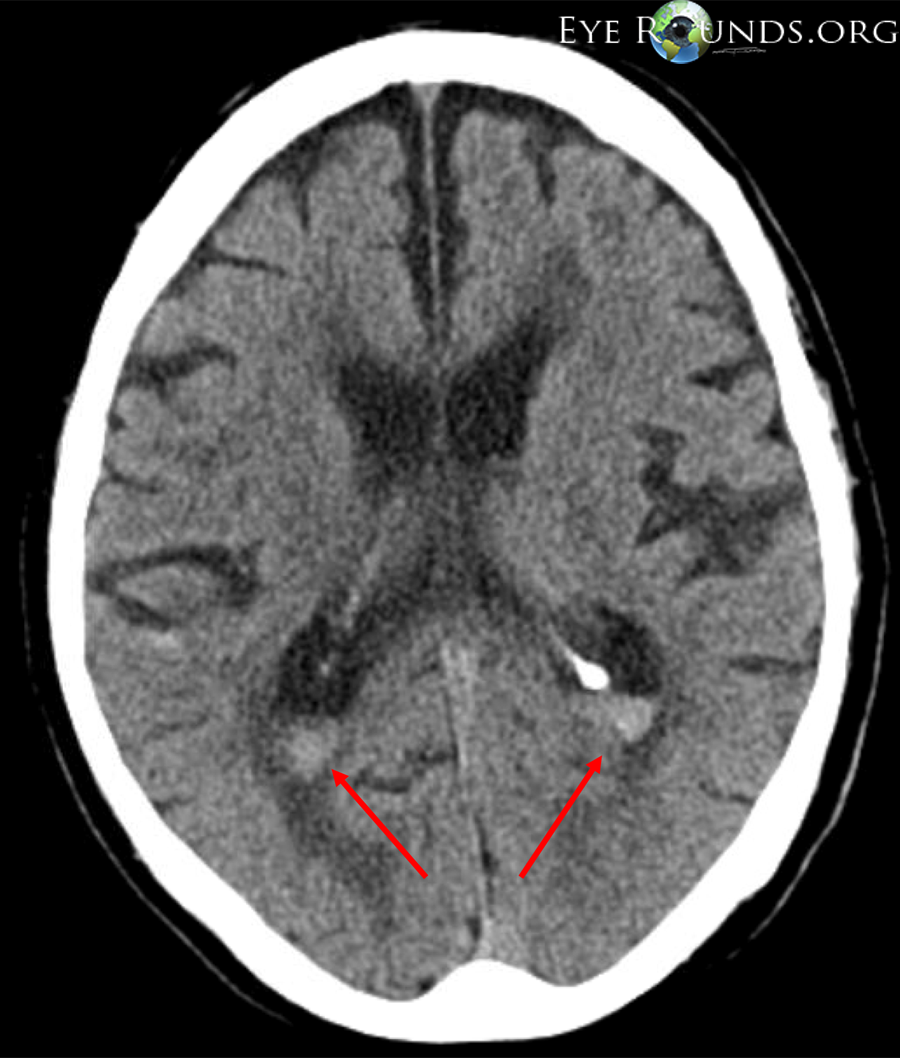 |
| Figure 5: Non-contrast head CT, axial view, showing hyperdense pituitary adenoma (more dense than typical pituitary adenoma on CT), suggesting fresh hemorrhage | Figure 6: Post-contrast T1 brain MRI, mid-sagittal view, showing relatively mild, patchy contrast enhancement of the same pituitary adenoma seen in Figure 5. Note motion artifact from altered mental status. | Figure 7: Non-contrast head CT, axial view, showing layered hemorrhages within bilateral lateral ventricles |
Compressive optic neuropathy/junctional scotoma secondary to pituitary adenoma
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Weed MC, Longmuir RA, Thurtell MJ. Pituitary Adenoma Causing Compression of the Optic Chiasm: 49-year-old white female with painless progressive vision loss. EyeRounds.org. September 9, 2013; available from https://eyerounds.org/cases/177-pituitary-adenoma.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
