
Total body rash with mucosal involvement
A 13-year-old female was prescribed trimethoprim-sulfamethoxazole by her primary care provider for a lower extremity infection. In the following days, she developed a fever of 103° F, conjunctival injection, and an erythematous rash involving >60% body surface area with bullae involving <10% body surface area. The antibiotic medication was immediately discontinued, but her symptoms continued to worsen. She was subsequently admitted to the pediatric critical care unit at the University of Iowa and diagnosed with Stevens-Johnson syndrome by dermatology. The ophthalmology service was consulted given her ocular involvement with Stevens-Johnson syndrome.
Past Ocular History: Noncontributory
Past Medical History: Recurrent upper thigh boils. Unremarkable workup per dermatology and allergy/immunology
Medications: Current admission — famotidine, hydromorphone, intravenous immunoglobulin (IVIG), ondansetron
Allergies: Codeine, sulfa
Family History: Maternal thyroid disease. Ocular family history is noncontributory.
Social History: Noncontributory
Review of Systems: Positive for fevers, eye irritation, cough, and rash. Otherwise negative
Mood/affect: Somnolent
External exam: Extensive bullae, sloughing of skin, and erythematous macules and patches
Mild, diffuse injection of the bulbar conjunctiva OU. The palpebral conjunctiva was markedly injected with conjunctival membranes bilaterally (Figures 1, 2)
Large, central epithelial defect involving 80% of the corneal surface on each eye
Normal
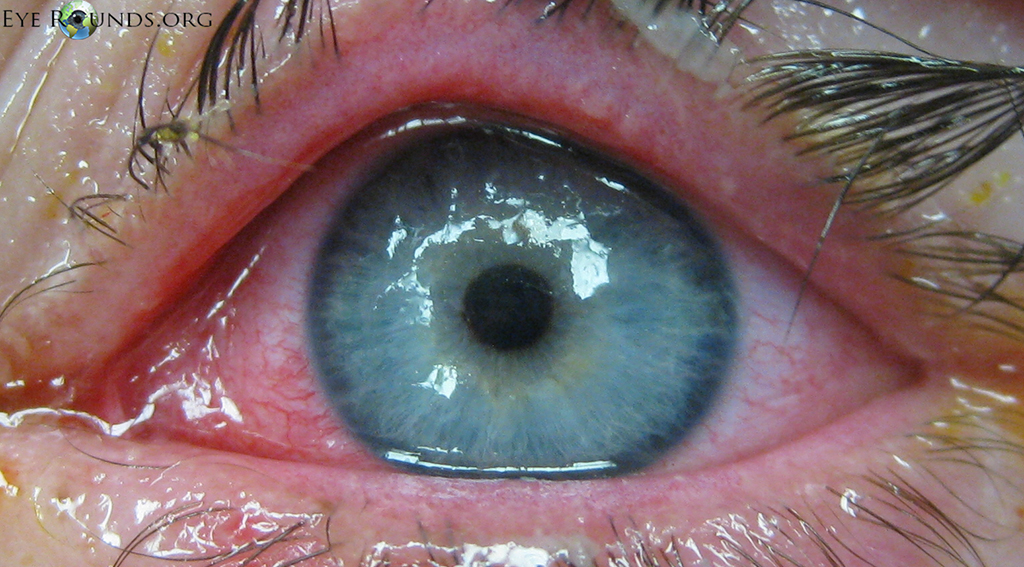
Figure 1. External photograph of the left eye showing a corneal epithelial defect and diffuse conjunctival injection
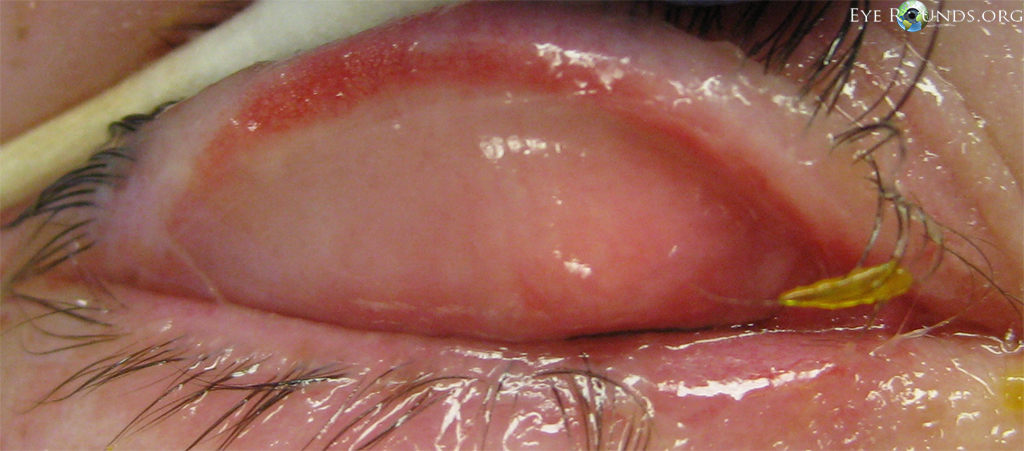
Figure 2. Eversion of the right upper eyelid shows a conjunctival membrane.
Given the significant ocular involvement, the patient underwent urgent bilateral amniotic membrane grafts to the upper and lower palpebral conjunctiva and placement of a ProKera® amniotic membrane ring. Post-operatively, the patient was treated with gatifloxacin and prednisolone drops and tobramycin/dexamethasone ointment. She was able to open her eyes comfortably on the first postoperative day and experienced rapid improvement of her ocular symptoms. There was complete resolution of the corneal epithelial defects at her three-week follow-up visit. By six weeks, she demonstrated 20/20 uncorrected visual acuity in each eye.
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are similar conditions characterized by intraepidermal cell death leading to diffuse vesicobullous eruptions. The differentiating criteria for SJS and TEN is the extent of skin detachment; SJS is defined as <10% total body surface area, SJS-TEN overlap as 10-30%, and TEN as >30%. Mucosal involvement is common, occurring in up to 90% of patients, and may involve the ocular surface in as many as 80% of patients [1]. The incidence of SJS/TEN is low at an estimated 1-7 cases per million per year [2].
The exact pathogenesis of SJS/TEN is unknown but appears to involve cell-mediated keratinocyte apoptosis via the Fas signaling cascade and granulysin release [3]. The syndrome can result from exposure to certain medications, infections, or malignancy, though almost a quarter of cases have no known trigger [4]. Medications are the most frequently implicated inciting factor with antibacterial sulfonamides, such as trimethoprim/sulfamethoxazole, and anticonvulsants, such as phenytoin, as the leading culprits. Infections are the next most common cause. There is an especially strong association with Mycoplasma pneumoniae in children, but other infectious causes of SJS/TEN are relatively rare. In addition, it is important to note that HIV patients have up to a hundred-fold increase in susceptibility, likely due to immunologic abnormalities and intensive drug regimens. Many other medications and infectious agents have been associated with SJS/TEN, but the most common etiologies are listed in Table 1.
Pharmacologic |
Infectious |
|---|---|
|
|
The disease can have severe sequelae. The prognosis varies with severity of disease, but the overall six-week mortality rate for patients on the SJS/TEN spectrum is 23%, arising from acute complications including severe fluid imbalances, infections, and respiratory failure. Mortality remains high even after resolution of the acute phase, with a one-year all-mortality rate of 34% [5].
Amongst survivors, long-term ocular complications can be serious and are thought to affect approximately 60% of patients [6]. Corneal damage in the form of scarring or limbal stem cell failure is the most severe ocular outcome. Conjunctival scarring can contribute to long-term corneal pathology and subsequent visual impairment (Figure 3). For example, palpebral conjunctival scarring can cause chronic microtrauma with the blink reflex, while symblepharon formation can lead to poor tear film dynamics and predisposition to severe dry eye [7].
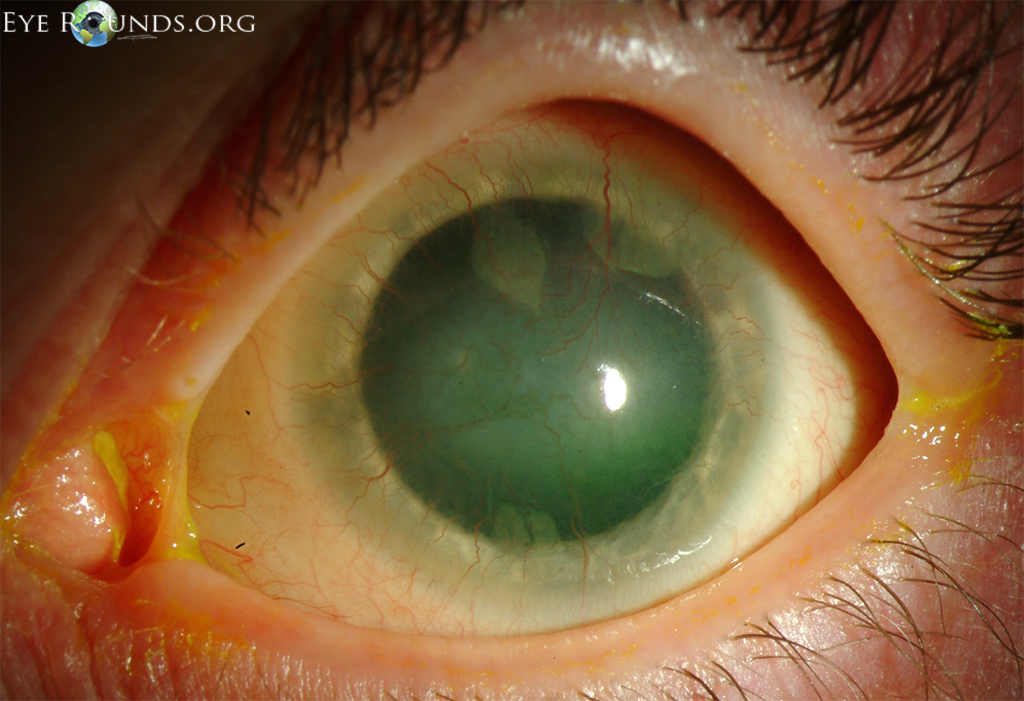
Figure 3. Slit-lamp photograph showing the long-term consequences of SJS/TEN, which can include limbal stem cell deficiency and symblepharon.
Because ocular involvement is common and there is potential for severe visual consequences, all patients with SJS/TEN should be urgently evaluated by an ophthalmologist. Fluorescein staining should be used to evaluate the extent of corneal and conjunctival epithelial defects. Close examination of the palpebral conjunctiva is a critical component of the examination as it is frequently affected by SJS/TEN.
While systemic corticosteroids are frequently used for the management of SJS/TEN, widespread acceptance of this approach has long been controversial. Evidence for its efficacy is lacking and early studies associate systemic steroids with a slight increase in the mortality of pediatric patients [8]. Intravenous immunoglobulin (IVIG), administered with the goal of inhibiting the Fas-ligand signaling pathway, has recently gained traction as a possible therapy but studies regarding its efficacy continue to have conflicting findings. Of note, one recent study found improved ocular outcomes associated with IVIG therapy compared to systemic steroids [9].
Studies investigating the therapeutic value of topical medications for ocular SJS/TEN are similarly lacking. While there is no standard treatment, a combination of topical corticosteroids and antibiotics are often used in cases of mild ocular involvement, with one retrospective study suggesting that early topical steroids are associated with improved visual outcomes [10]. For more severe ocular involvement, there is evidence that early surgical intervention with amniotic membrane can lead to improved outcomes [7, 11, 12].
The amniotic membrane (AM) is the innermost layer of the placenta and is comprised of a thick basement membrane with a poorly cellularized stromal matrix. Its value in ophthalmologic surgery lies in its ability to enhance epithelialization, reduce inflammation, inhibit neovascularization, and prevent ocular surface scarring. AM delivers a complex signaling milieu comprised of immunomodulators and growth factors, while simultaneously providing a substrate for epithelial cell growth [13]. It may be used as either a temporary bandage or permanent graft. The ProKera® device consists of an amniotic membrane sheet attached to a polycarbonate ring and is designed for use as a temporary bandage for corneal and perilimbal lesions. This is an easier alternative to directly suturing AM to the bulbar conjunctiva, a technique seen in Video 1 below, but both methods have demonstrated excellent ocular outcomes [11].
The use of amniotic membrane transplantation (AMT) for SJS/TEN was first reported in 2002 with subsequent studies supporting its effectiveness in minimizing long-term visual sequelae [7]. These studies emphasize the importance of early AMT intervention. Outcomes are patient-dependent, but results indicate that delays in treatment beyond 5 to 10 days after rash onset are associated with decreased visual acuity and increased ocular complications [11, 12]. In addition, AM coverage of the entire conjunctival surface is crucial to maximizing benefit; patients undergoing AMT only to the bulbar conjunctiva may still develop the chronic sequelae of SJS/TEN [12].
Not every case of SJS/TEN is suitable for AMT. This technique is generally reserved for patients with moderate or severe conjunctival involvement, as these are the patients at greatest risk of visual loss from ocular surface scarring. Patients with minimal epithelial sloughing may instead be treated medically.
If Video fails to load, use this link: Fornix Reconstruction with Amniotic Membrane
Video 1: Surgical technique for amniotic membrane transplantation. AM is sutured directly to the bulbar conjunctiva. The upper and lower palpebral conjunctiva is then covered with AM and sutured at the lid margins.
Though intervention in the acute stage has the best ocular outcomes, treatments also exist for the chronic sequelae of SJS/TEN. Keratoprosthesis and limbal allografting rarely match the success of early surgical treatment, but these methods can provide some visual recovery despite limbal stem cell loss and corneal conjunctivalization.
Patients with cicatrizing diseases, including SJS/TEN, are poor candidates for traditional penetrating keratoplasty (PKP) due to the development of lid abnormalities and severe surface dryness. For these eyes, the Boston keratoprosthesis (KPro) is an artificial cornea that may be used as a PKP alternative. There are two variations: the type I design (Figure 4) is sutured to the cornea in a similar manner as a PKP, while the type II design (Figure 5) is inserted through the upper lid following a permanent tarsorrhaphy. The type II is reserved for patients with severe surface disease, including symblepharon and poor surface wetting. The KPro has found some success in the treatment of chronic SJS/TEN, with studies reporting 75% of treated eyes achieving visual acuity >20/200 and 50% attaining >20/40 [14]. Experience with the KPro at the University of Iowa has also been promising, demonstrated by one patient sustaining 20/25 vision for four years following implantation.

Figure 4. Outcome of Boston KPro type I for corneal conjunctivalization. This patient attained 20/25 vision following surgery.
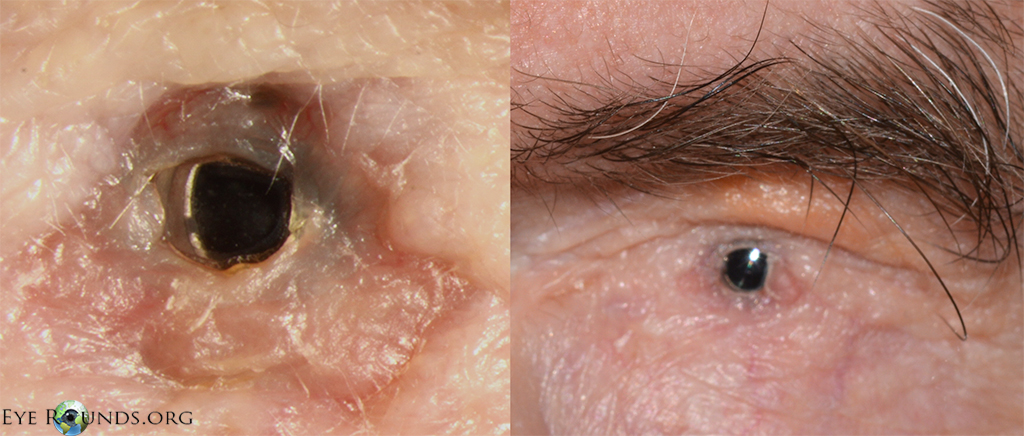
Figure 5. Boston KPro type II, selected over the type I design due to severe ocular surface dryness and symblepharon formation following SJS/TEN. The optic can be seen protruding through the upper eyelid while the eyelids are closed with a complete tarsorrhaphy.
Keratolimbal allografting (KLAL) is a technique that transplants cadaveric keratolimbal tissue to correct limbal stem cell deficiency. Early studies examining KLAL as a treatment of chronic ocular SJS were discouraging, as only 30% of eyes maintained visual acuity >20/200 at two-year followup [15]. This sub-optimal outcome, along with the need for chronic systemic immunosuppression, renders the KLAL-only approach an inferior treatment option. However, when a modified KLAL technique is followed with KPro implantation, 90% of eyes demonstrate improved vision [16]. Thus, limbal allografting may have a role in enhancing the visual outcomes of the Boston KPro in chronic SJS/TEN patients.
Epidemiology
|
Signs
|
Symptoms
|
Treatment
|
Wang, JW, Rixen JJ, Goins KM, Kitzmann AS. Ocular Manifestations of Stevens-Johnson Syndrome: 13-year-old female with mucosal and dermatologic eruptions. EyeRounds.org. August 20, 2014; available from https://eyerounds.org/cases/192-Stevens-Johnson.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
