Pigmented iris lesion of the left eye
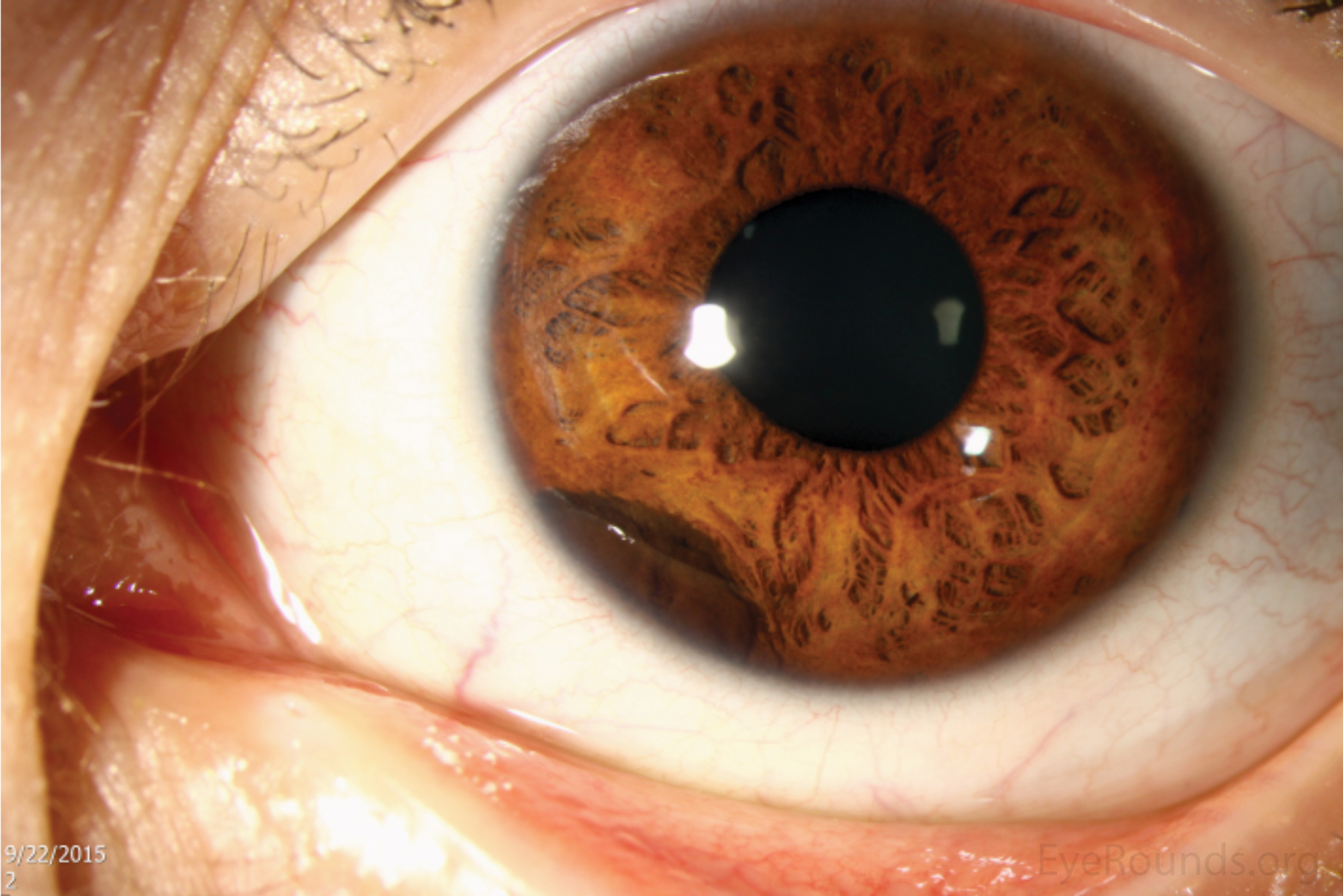
A 14-year-old male was referred for evaluation of a pigmented iris lesion of the left eye that was noticed on routine eye exam approximately two years prior. The lesion has reportedly not grown or changed in appearance since initial discovery. He denies vision changes, ocular pain, flashes, floaters, and photophobia. He denies sensation of ocular pressure and headaches.
 |
 |
 |
 |
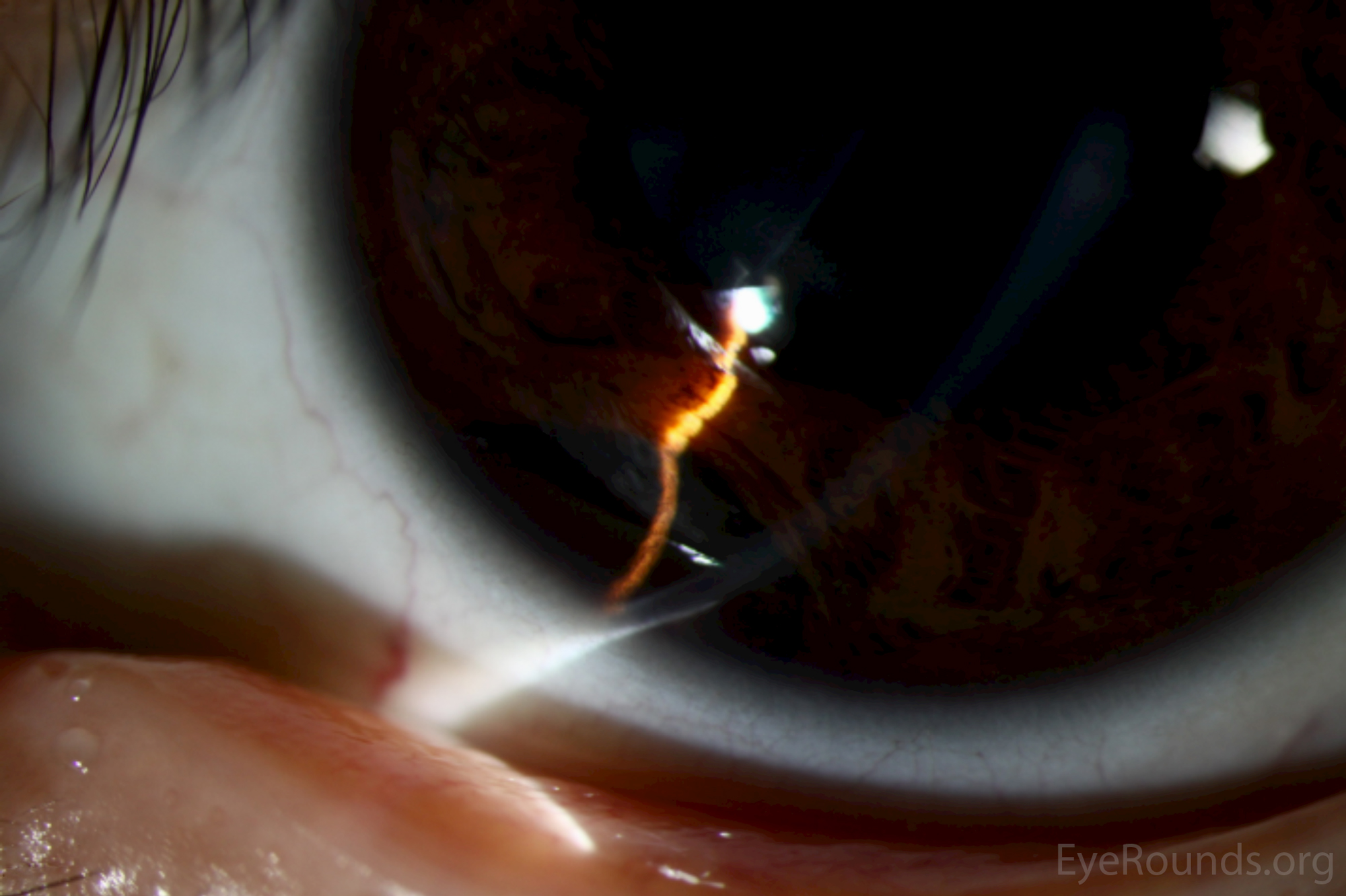
Video 1: Slit lamp examination demonstrating findings described above.
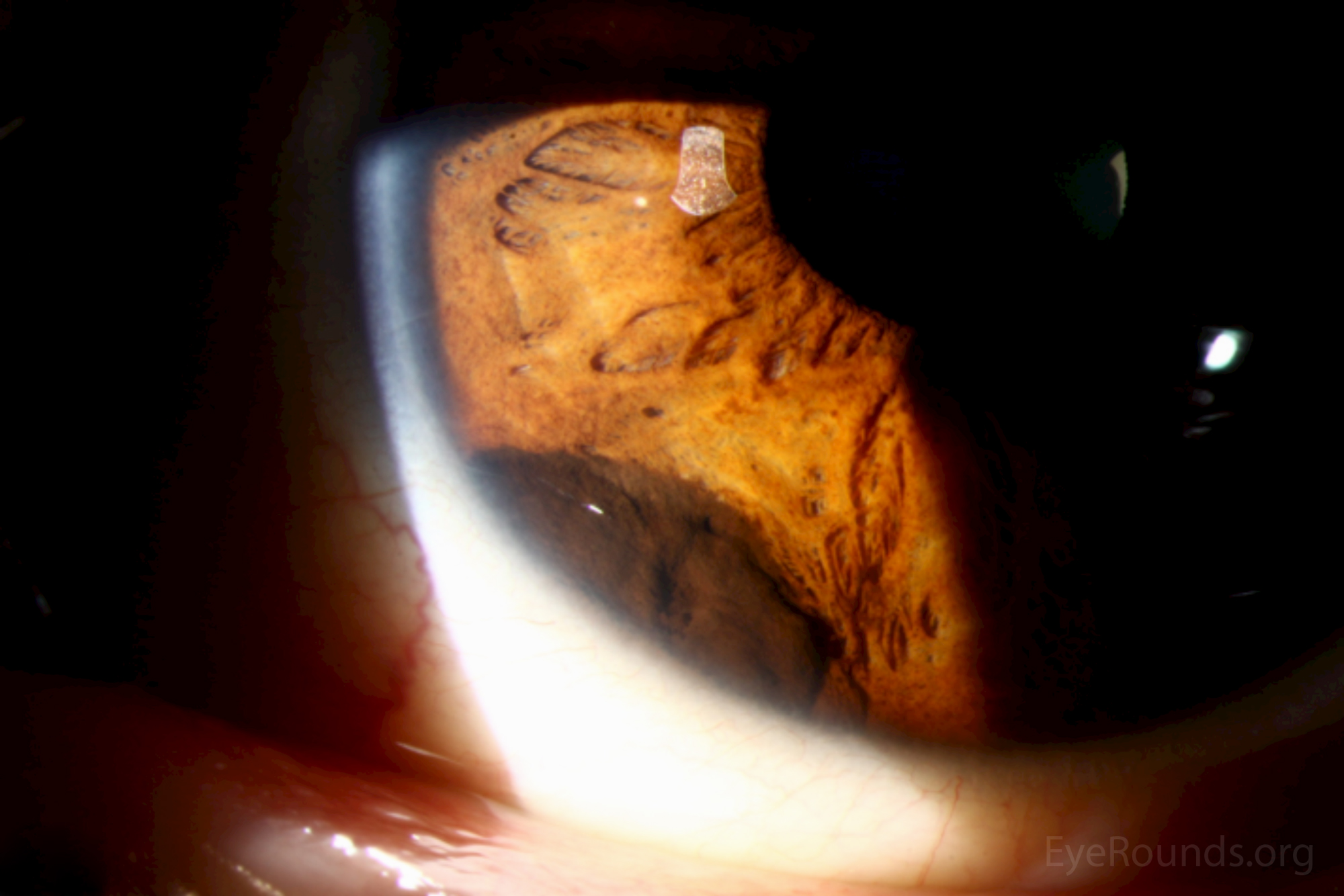
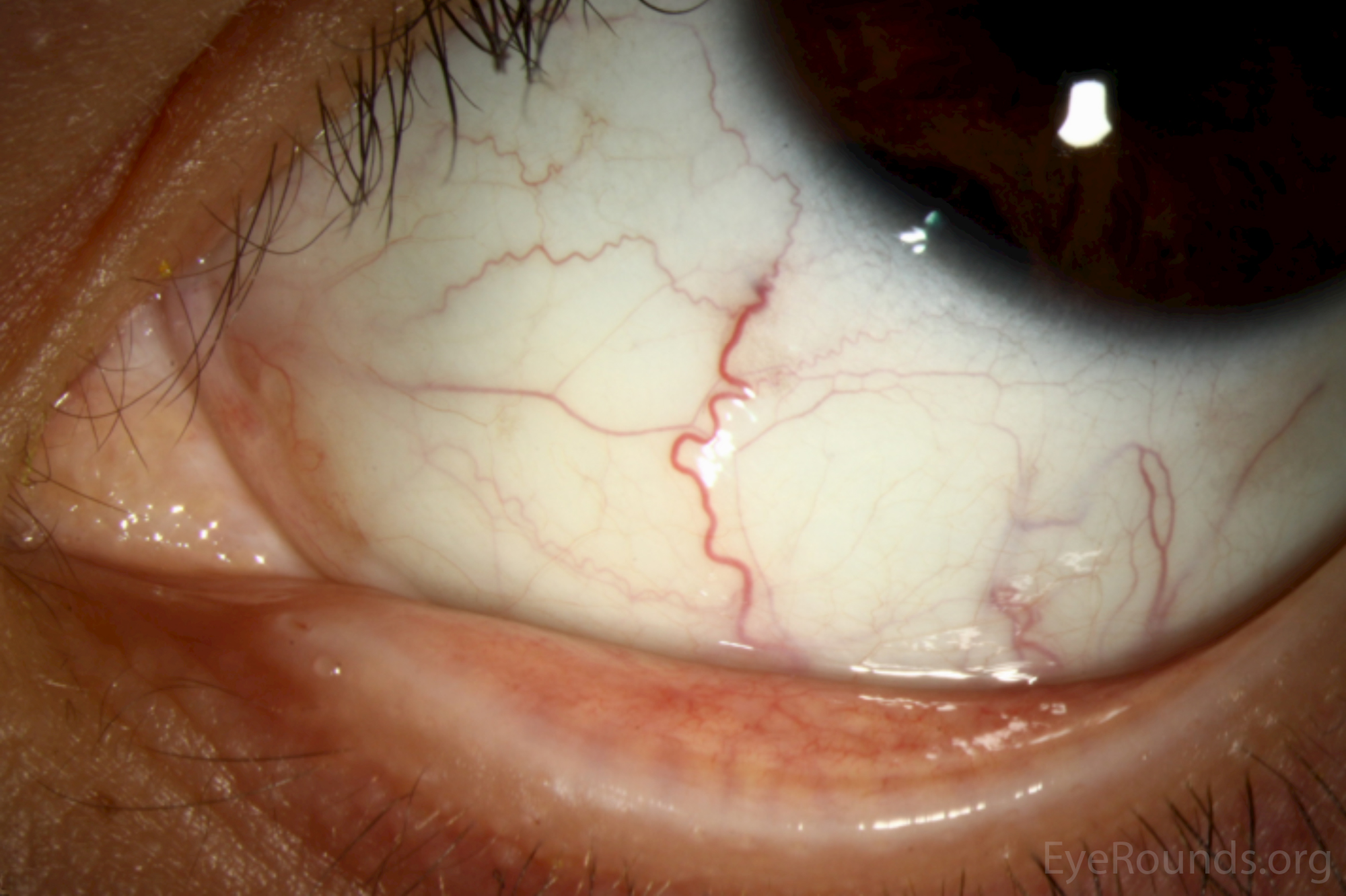
Figure 2: On gonioscopy, an elevated, dark brown lesion is seen extending from 7 to 8 o'clock without spread into the surrounding trabecular meshwork.
Video 2: Gonioscopy examination demonstrating findings described above.
 |
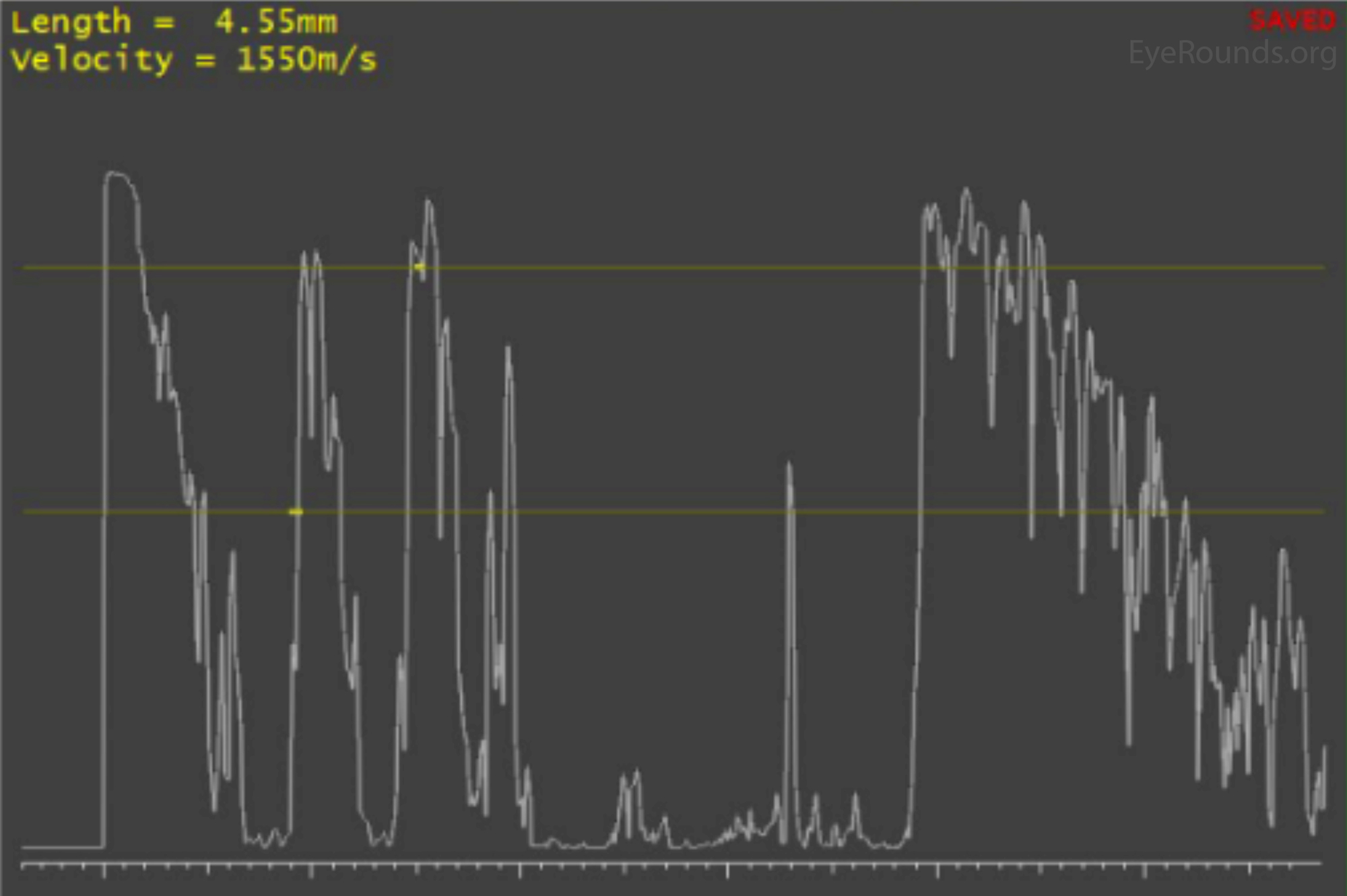 |
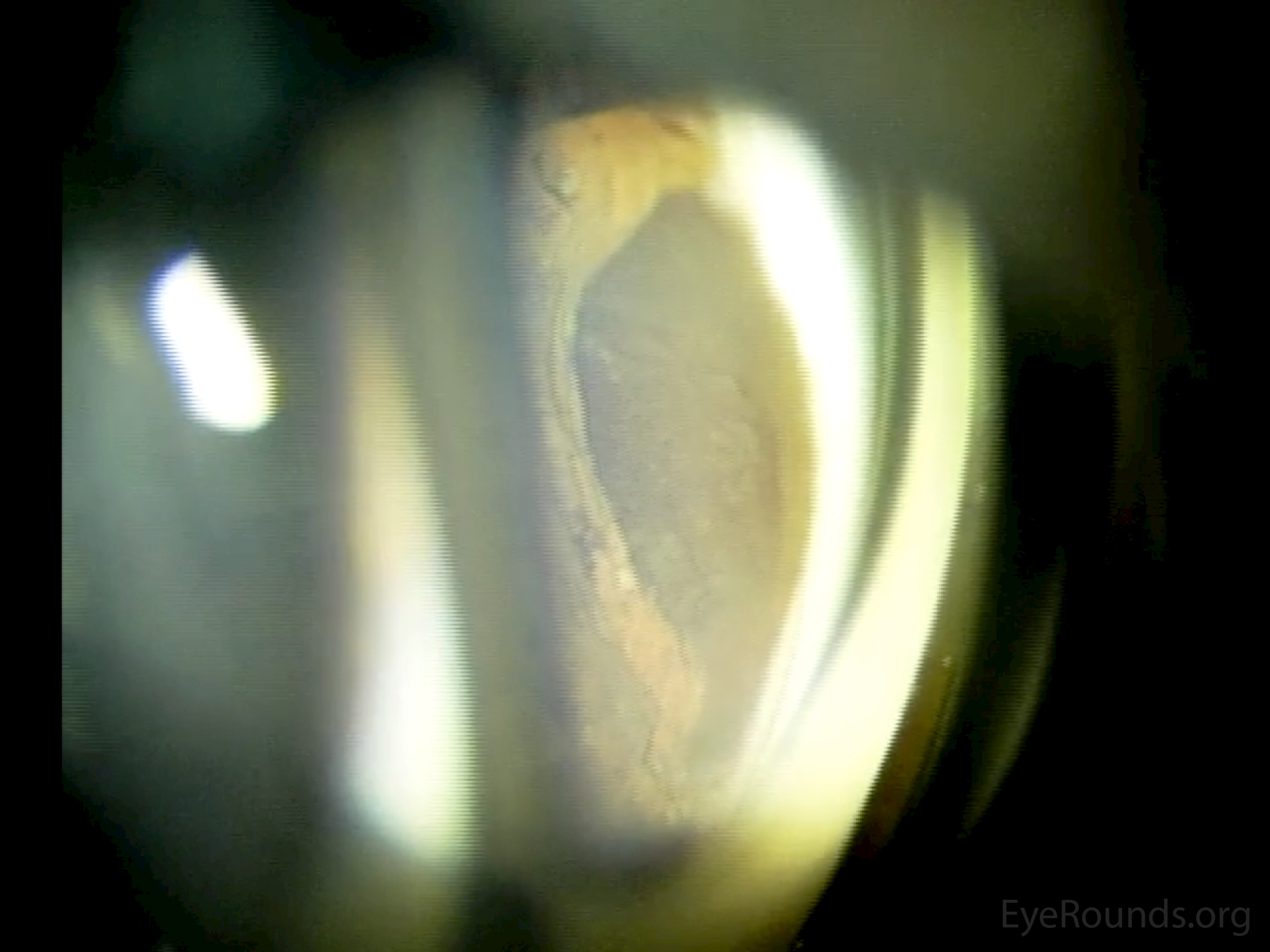
Figure 4: Photo of infrared iris transillumination revealing an oval-shaped area of blockage at the inferonasal corneoscleral limbus.

Video 3: Video of infrared iris transillumination demonstrating same limbal intraocular mass as seen in Figure 4.
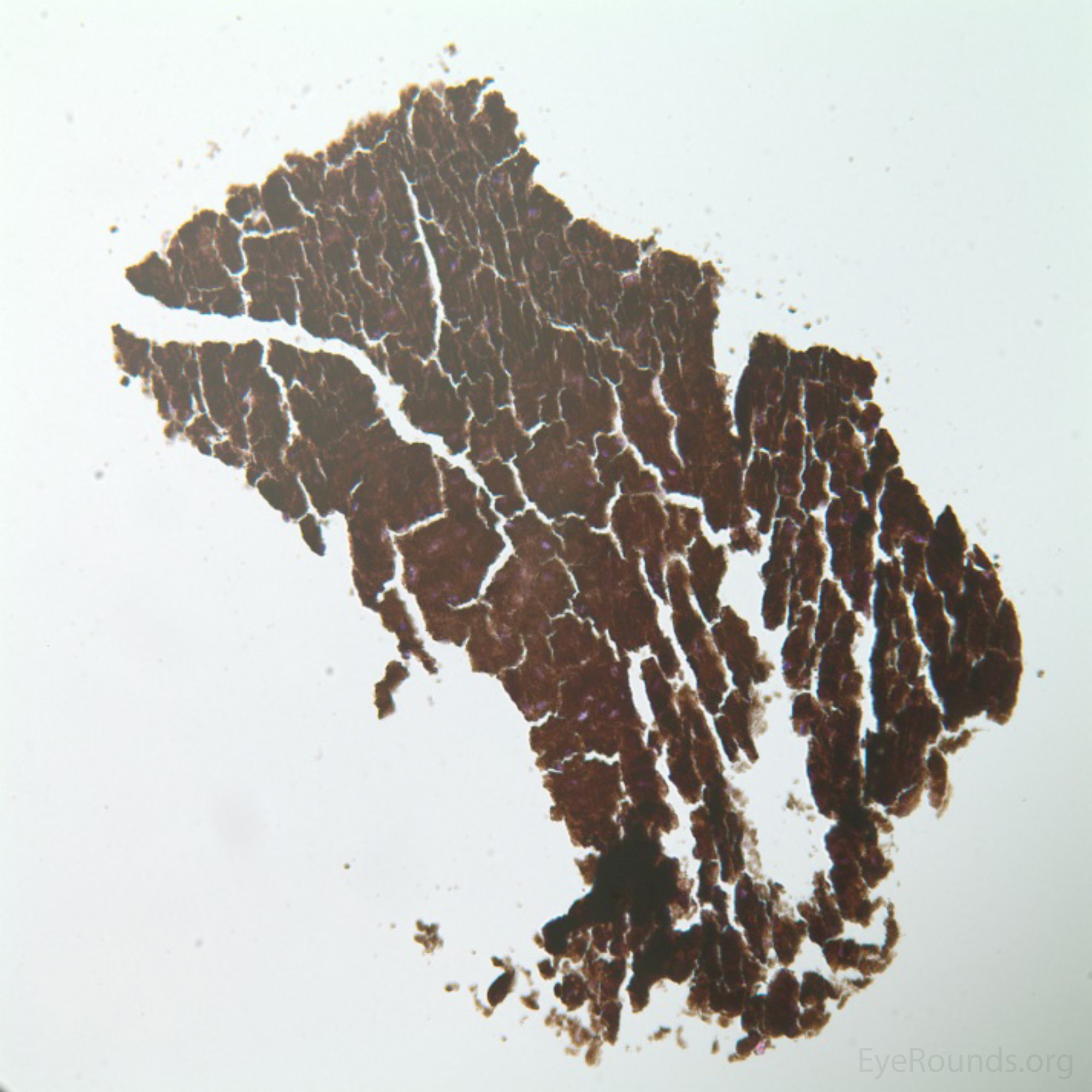
A fine-needle aspiration biopsy (FNAB) of the lesion was performed under general anesthesia.
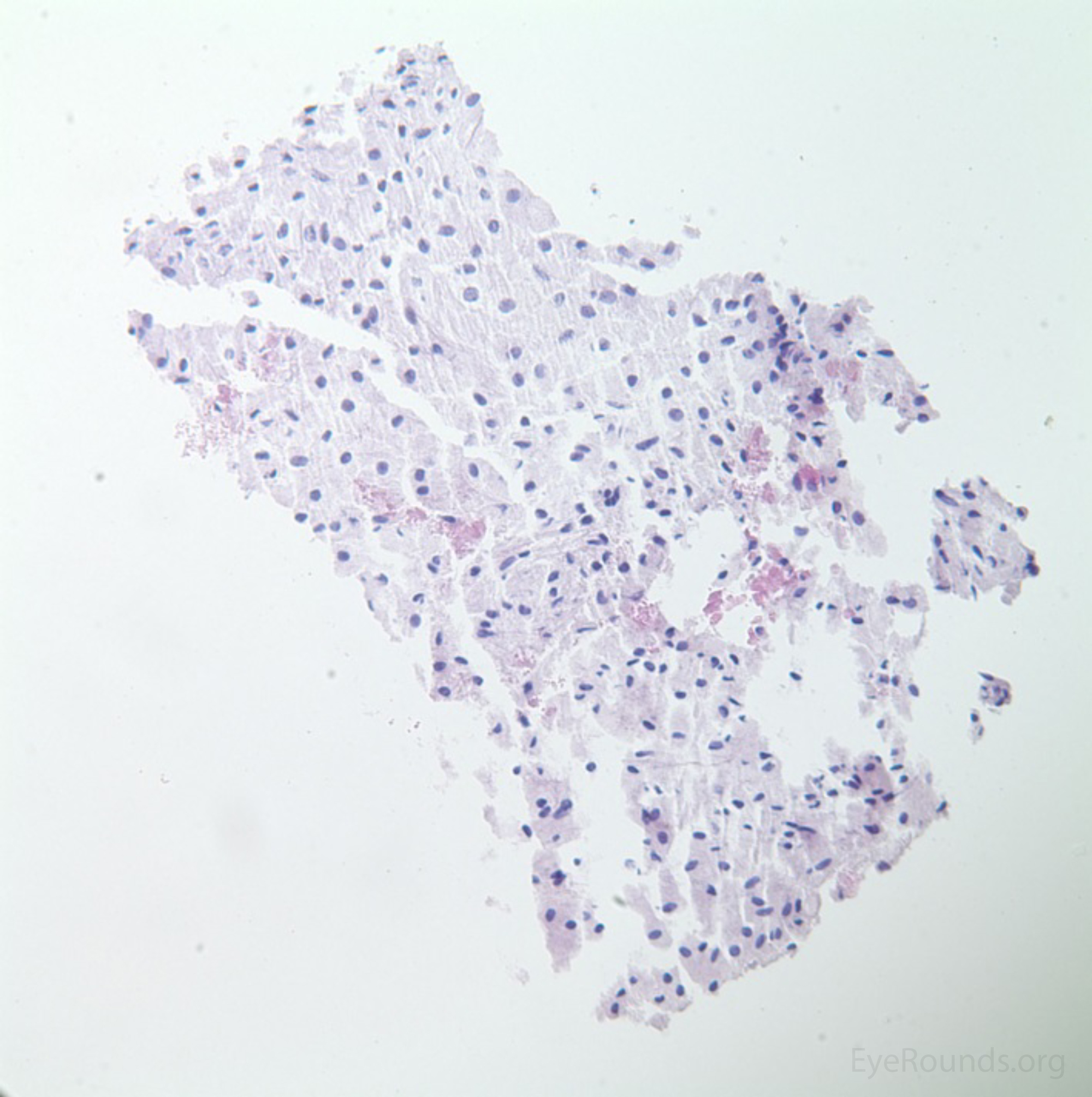
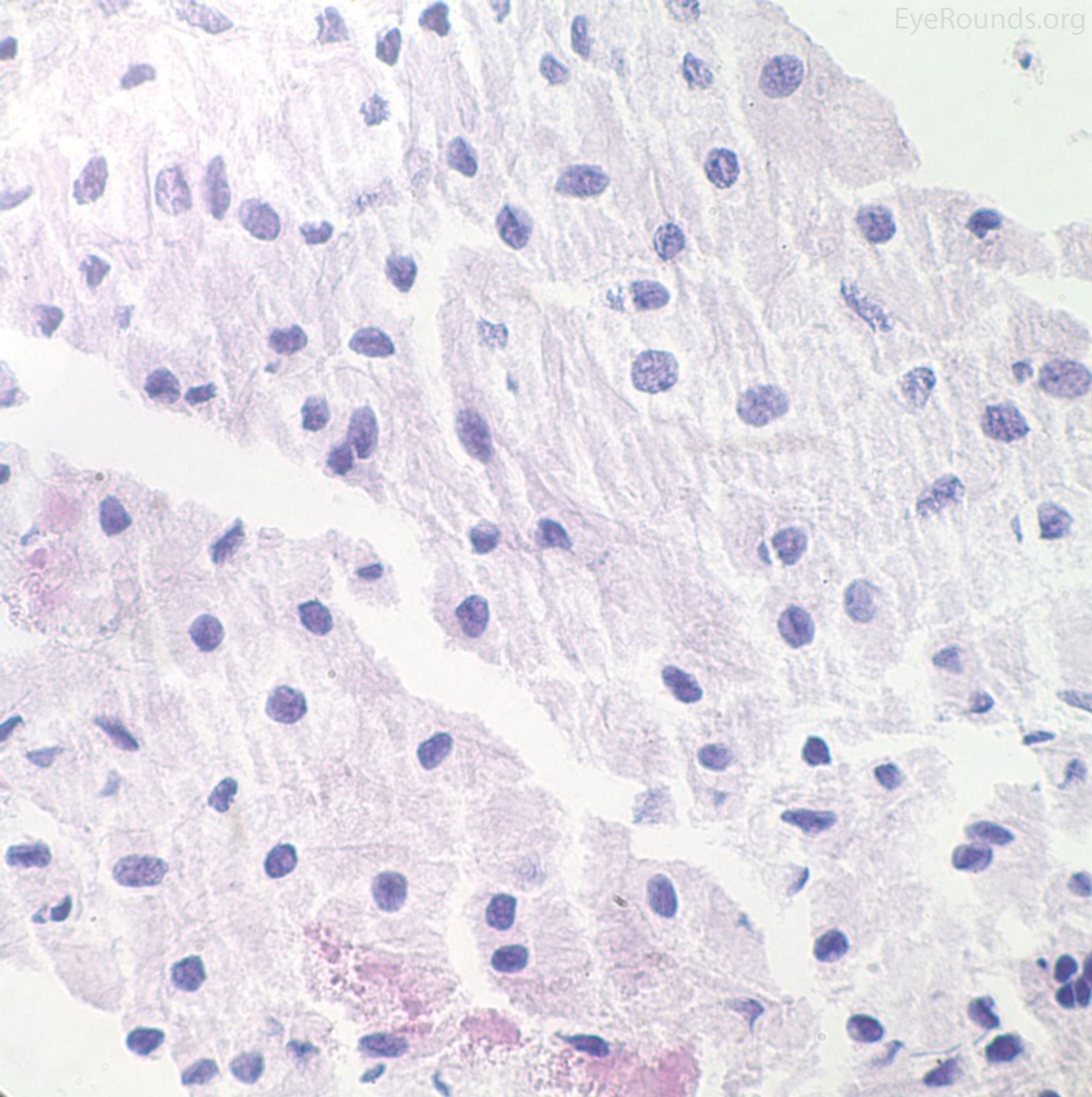
Histologic examination demonstrated fragments consisting of heavily pigmented cells, with the pigment obscuring all cellular details. Melanin bleach hematoxylin and eosin (H&E) stain revealed that the tissue fragment was composed of large, polygonal cells with bland nuclei and abundant cytoplasm consistent with the diagnosis of melanocytoma.
 |
 |
|
 |
Post-biopsy, management options were discussed with the patient and his family. Surgical excisional biopsy was discussed as an option along with the potential complications, such as cataract and retinal detachment. The low risk of future malignant transformation was discussed. The alternative of observation was also discussed. Ultimately, the patient and his family elected for serial observation with photography and ultrasound biomicroscopy over surgical intervention.
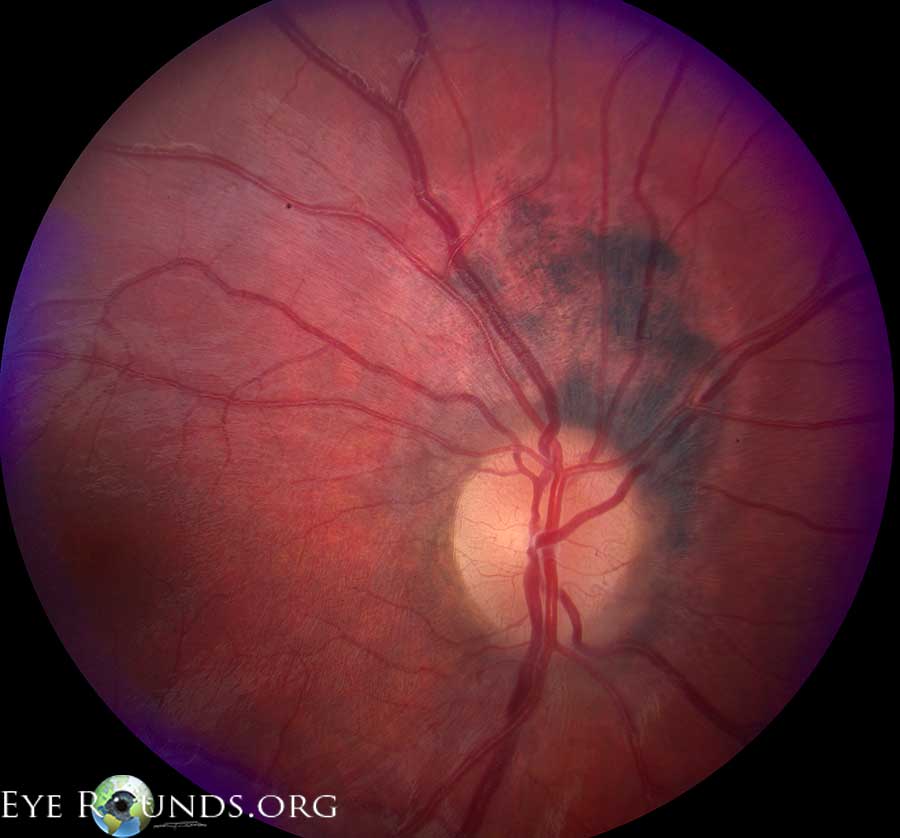
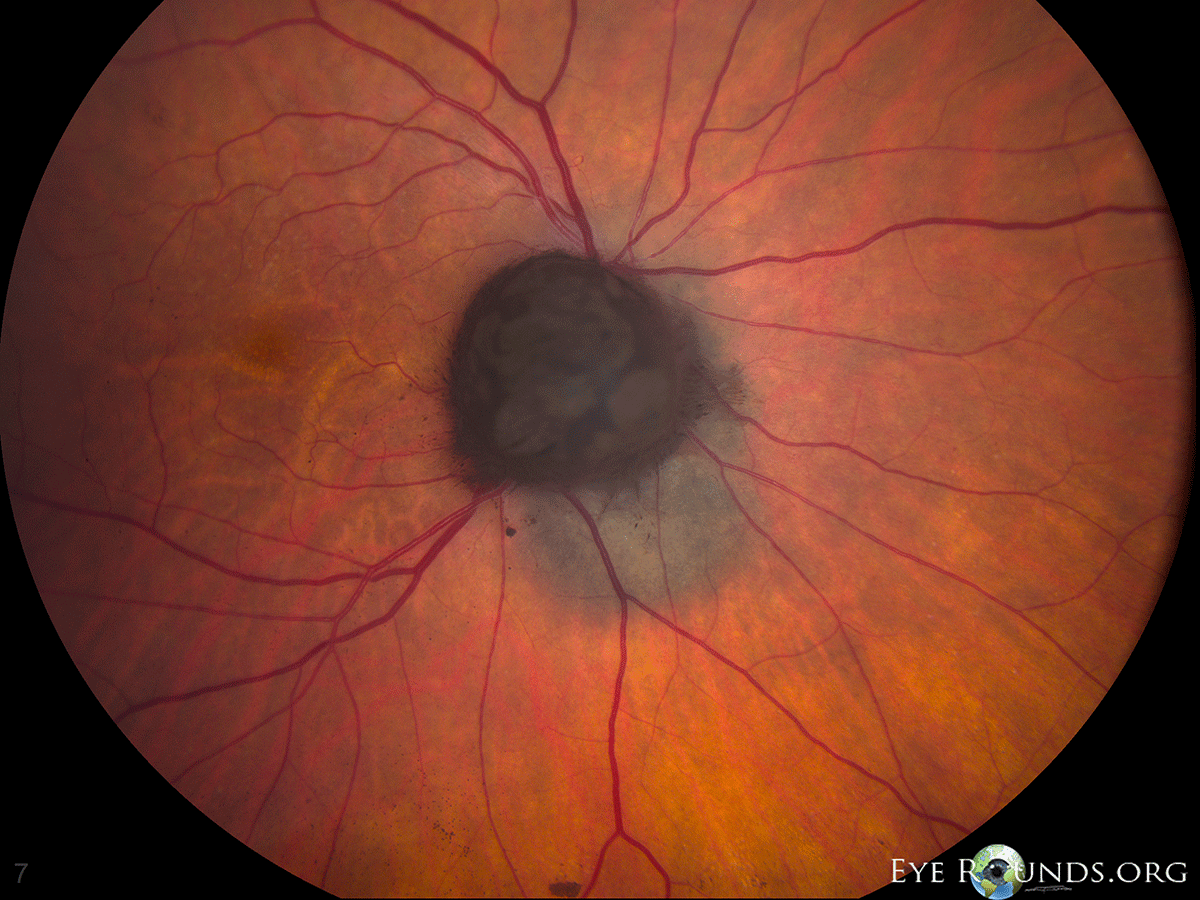
Melanocytoma is a type of uveal tract nevus, also known as "magnocellular nevus," characterized clinically by its jet-black coloration and histologically by its heavily pigmented, large, polygonal, bland cells.[1] Melanocytomas most often present as asymptomatic pigmented lesions, although an isolated case of painful melanocytoma involving the ciliary body and iris root has been reported. [2] Melanocytomas can occur anywhere along the uveal tract, but are most commonly found in the juxtapapillary region of the choroid where they appear as elevated, pigmented masses and are sometimes mistaken for a typical choroidal nevus or choroidal melanoma. Melanocytomas arising in the ciliary body are usually detected late given their anterior location and are most commonly confused with ciliary body melanomas. They may be detected on dilated fundus examination, gonioscopy, or on slit lamp examination if an anterior growth phase results in extension into the anterior chamber angle. In rare cases, a ciliary body melanocytoma can extend through a scleral emissary canal and present as a pigmented, subconjunctival mass.
Figure 6a: Melanocytoma |
Figure 6b: Melanocytoma with associated choroidal nevus |
Melanocytomas of the iris present as pigmented lesions with "mossy" or irregular surface that may involve the anterior chamber angle. [3] In a published case series of 47 iris melanocytomas, presenting symptoms included: patient discovery of a pigmented spot (15%), blurry vision (11%), and conjunctival hyperemia (4%). [3] Seventy percent of cases were asymptomatic. [3] In this same series, 85% of iris melanocytomas were nodular and 15% diffuse; they were typically located in the inferior (45%) or temporal (38%) quadrants. [3] Iris heterochromia was seen in 13% of cases, a sentinel vessel in 15%, satellite tumors with angle involvement (mean of 8 clock hours) in 26%, and ectropion uvea in 6%. [3] Less than 5% of patients presented with increased intraocular pressure (IOP). [3] The differential diagnosis of iris melanocytoma is listed below in Table 1. Notably, iris melanocytomas may mimic the Cogan-Reese variant of iridocorneal endothelial (ICE) syndrome due to the potential for a rise in IOP in the presence of iris abnormalities. [4,5] The IOP rise associated with iris melanocytoma is presumably caused by clogging of the trabecular meshwork by liberated melanocytoma cells and/or pigment-laden macrophages. [3,5]
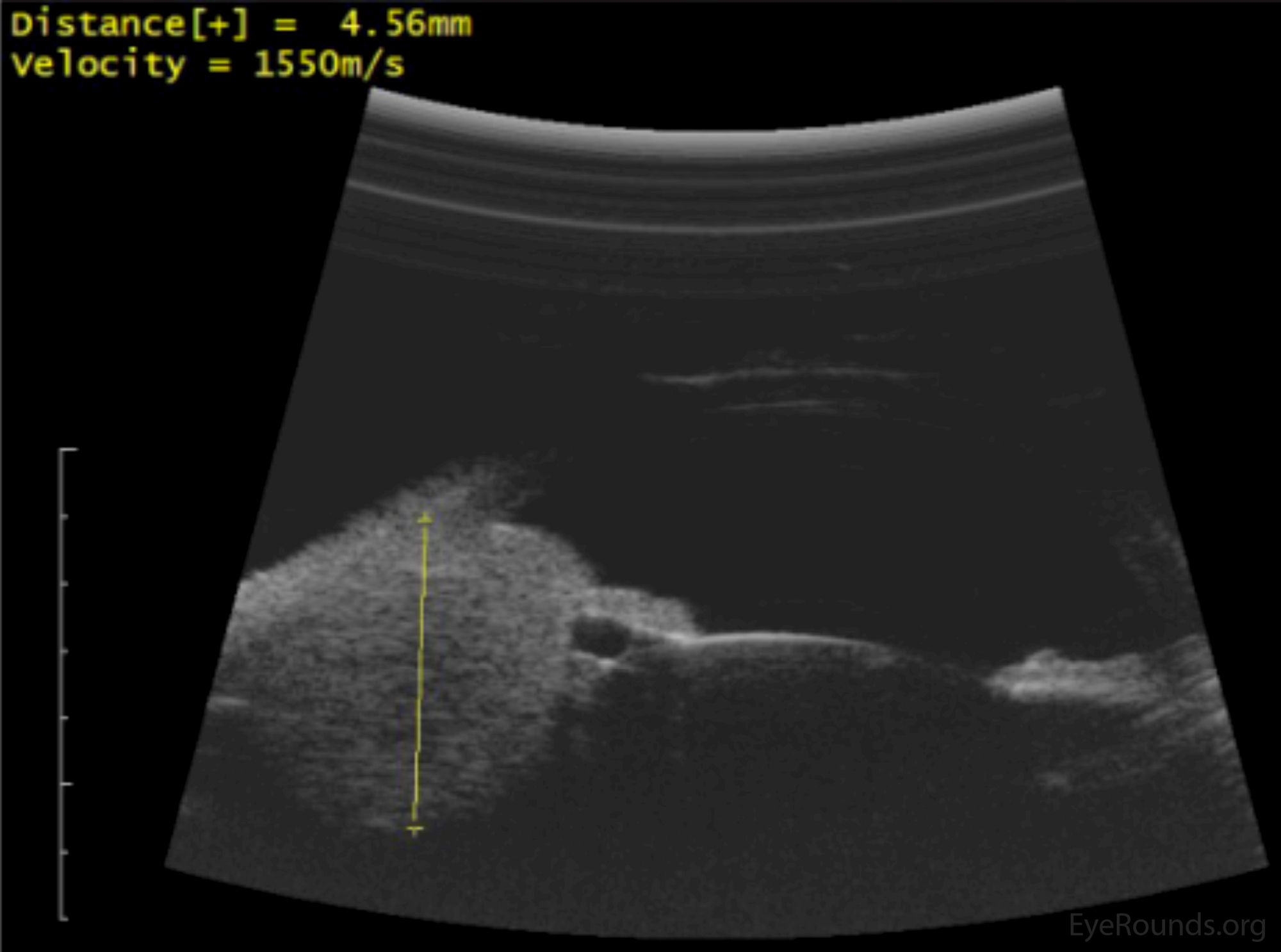
High frequency anterior segment ultrasound biomicroscopy is a useful modality in the workup of a pigmented iris lesion, as benign cystic lesions (e.g. iris pigment epithelial cysts) are readily differentiated from more worrisome solid mass lesions. Ultrasound biomicroscopy is also helpful in delineating the degree of posterior extension (i.e. the presence of ciliary body and/or choroidal involvement) of the lesion in question. Infrared iris transillumination is an additional imaging modality that can be utilized to determine the size and extent of a solid mass lesion. B-scan ultrasonography is helpful with lesions demonstrating posterior extension. On ultrasound biomicroscopy, melanocytomas are typically seen as highly-reflective nodular masses with a smooth or irregular surface and sharp, well-defined edges. [6] However, these characteristics are not pathognomonic for melanocytoma.
A physician may elect to observe a pigmented iris mass for signs of growth if the size, consistency, margins, and imaging are not overtly concerning for malignancy. However, when diagnostic uncertainty remains following clinical examination and imaging, tissue diagnosis can prove definitive. [1,7] While many pigmented iris lesions are able to be carefully and closely observed, biopsy is typically pursued when growth is documented, when noninvasive diagnostic techniques fail to establish the diagnosis, or when further observation poses danger to the patient, the eye, or the visual acuity. [3,8] Fine needle aspiration is the least invasive and most commonly utilized method of tissue procurement. The utility of FNAB has been debated with some authors strongly advocating its use and others criticizing the technique due to potentially false reassurance. [8,9,10] Complications from iris biopsy such as persistent hyphema, hypotony, lens damage, or endophthalmitis are rare with reported rates of less than 1%. [11] The risk for tumor seeding with transcorneal FNAB is largely theoretical and considered to be extremely low. [12] Histologically, melanocytomas are composed of large, plump, polygonal cells, with an abundance of cytoplasmic pigmentation that often obscures all cellular details and requires a melanin bleach stain in order to adequately assess with light microscopy. [1]
The management of iris and ciliary body melanocytomas is based upon the size of the lesion, associated complications (e.g. increased IOP, angle closure), and risk of possible malignant transformation. Treatment options most commonly include serial surveillance with routine photography and ultrasonography versus surgical excision (i.e. iridocyclectomy). [3,7] In the case of very large lesions, iridocyclectomy may be favored as further growth may render the lesion too large to be readily excised. Other indications for surgical intervention include progressive angle closure resulting in difficult to manage ocular hypertension/glaucoma and physical subluxation of the lens. [3,5] When extrascleral extension is present, en bloc excision with simultaneous full-thickness corneoscleral resection and patch graft placement has been shown, in a small case series, to be as effective as enucleation in terms of recurrence rates. [11]
Video 4. Iridocyclectomy, removal of a mass suspected of being malignant melanoma on the iris and ciliary body
The natural history of iris melanocytomas is variable. Spontaneous necrosis with resultant pigment dispersion and secondary glaucoma is rare, but has been reported. [13-20] A large case series of 47 eyes, revealed increased IOP in 0% of affected eyes at 1 year, 11% at 5 and 10 years, and 55% at 15 years. [3] This same series reported documented growth rates of 23% at 5 years, 48% at 10 years, and 74% at 15 years. [3] Transformation into a malignant melanoma is a rare event, with a reported occurrence rate of 2% for melanocytomas of the optic disc and rates even lower for iris melanocytomas. [3,21,23,24] However, given the life-threatening nature of malignant transformation, routine surveillance of all patients with a diagnosed melanocytoma is recommended. [21] In the case that malignant transformation is suspected, as evidenced by aggressive growth and/or change in appearance, the lesion should be treated as such with aggressive measures (e.g. surgical excision, enucleation, brachytherapy, or proton beam radiotherapy).
Melanocytoma of the iris and ciliary body is a rare, yet important diagnosis in the differential of a pigmented iris lesion. Melanocytomas are benign lesions, but do have the rare potential for malignant transformation. The diagnosis may be possible with clinical examination and imaging studies, but commonly requires histopathologic confirmation to rule out more worrisome diagnoses (e.g. melanoma or metastatic disease). Melanocytomas of the iris and ciliary body can be managed with serial observation, photography and ultrasonography, or surgically with iridocyclectomy or en bloc excision. Suspicion for malignant transformation warrants prompt and aggressive treatment.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Table 1: Differential diagnosis for an iris mass
Evans JA, Clark TJE, Syed NA, Alward WLM, Boldt HC. Melanocytoma of the Iris and Ciliary Body. EyeRounds.org. posted March 3, 2016; Available from: http://www.EyeRounds.org/cases/232-melanocytoma.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links