
"Poor vision in the right eye"
A 51-year-old pseudophakic female presents with poor vision in the right eye (OD). Fluctuations in vision were first noticed 6 months ago with documented vision as poor as 20/150. She had uneventful cataract surgery 10 years prior with insertion of a Polymethyl methacrylate (PMMA) intraocular lens (IOL) in the capsular bag. Until 6 months ago, the patient's best corrected vision OD had been stable and in the 20/25 range.
Video of slit lamp exam of a similar case by Dr. Lee Alward, Dr. Elliott Sohn, and Dr. Tom Oetting. If video fails to load, use this link: https://www.facebook.com/cataract.surgery/videos/10152780956891868/
 |
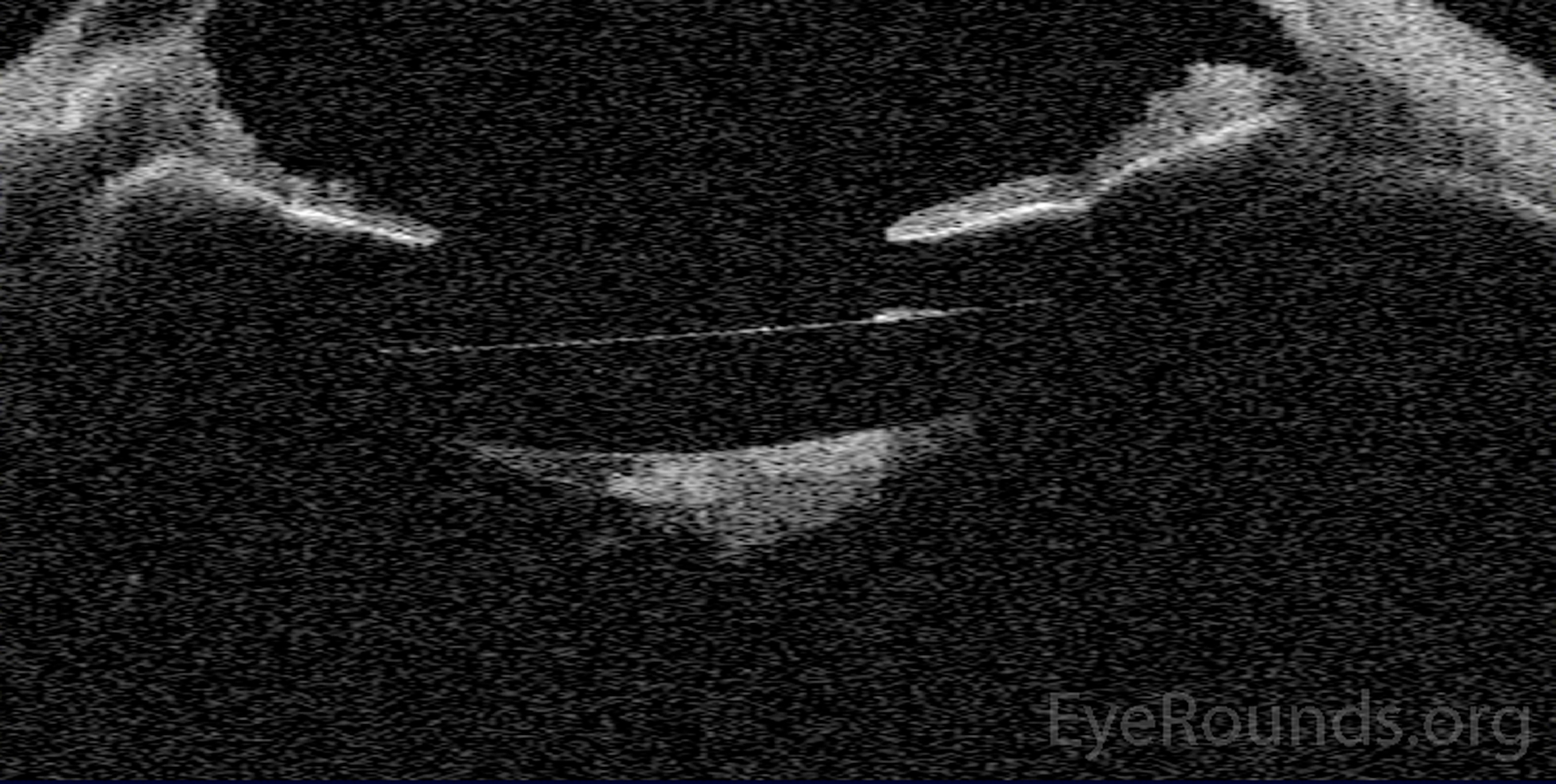 |
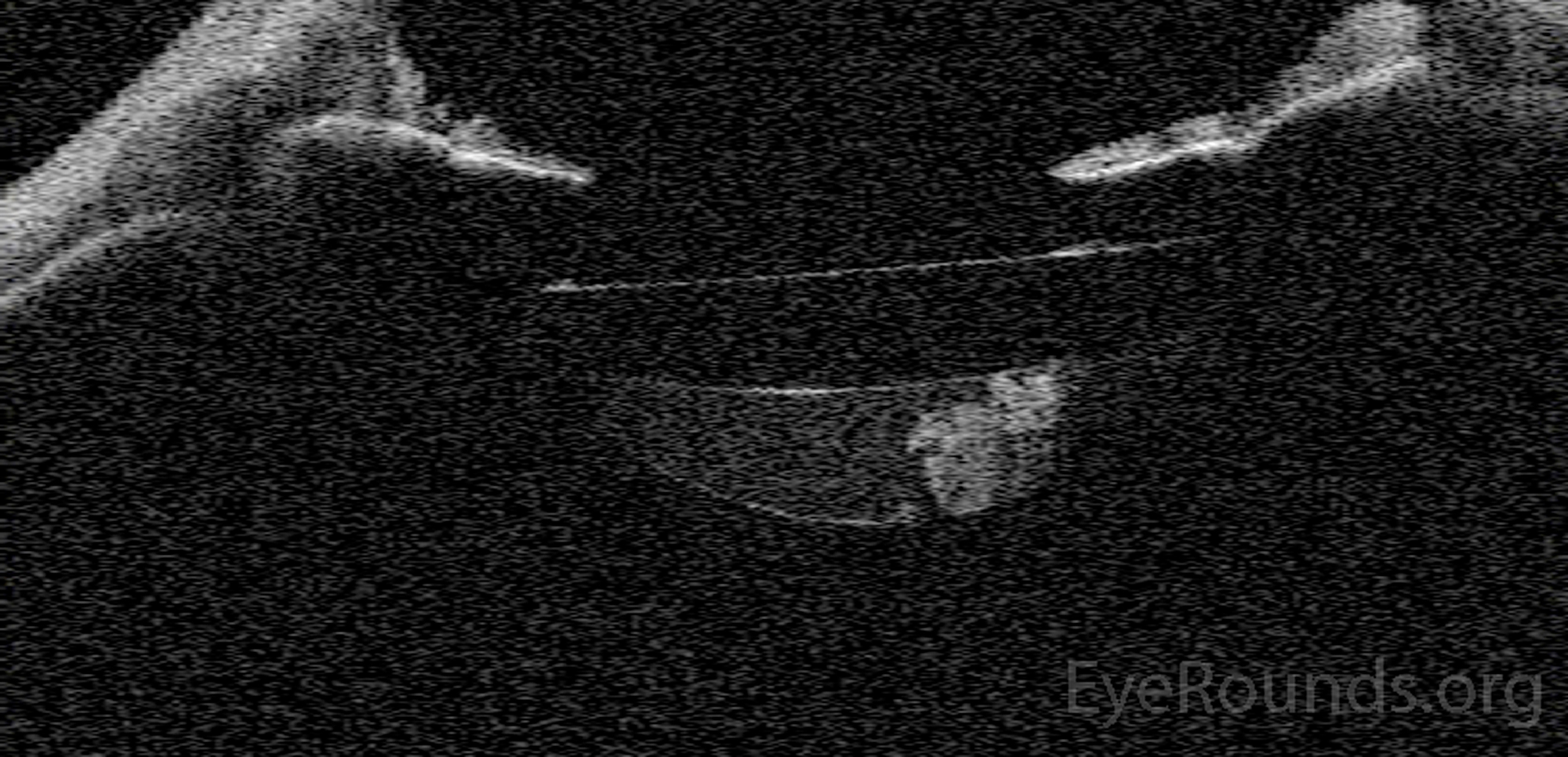
Figure 1. An anterior segment optical coherence tomography (AS-OCT) of the right eye demonstrates late capsular block pre-YAG capsulotomy (A), and post-YAG capsulotomy (B). Prior to capsulotomy, the capsular bag was distended with turbid fluid and lens material. Following capsulotomy, the turbid fluid is released with collapse of the space posterior to the lens. Occasionally, although not evident here, AS-OCT can demonstrate forward displacement of the lens optic during capsular block prior to YAG capsulotomy
This patient had Nd:YAG laser posterior capsulotomy to release distended fluid from the capsular bag and collapse the posterior capsule. Unfortunately, a collection of compressed residual lens material was pushed into the visual axis. Two subsequent YAG capsulotomies were performed to disrupt the residual lens material and clear the visual axis. Following this treatment, her myopic shift resolved and visual acuity returned to her baseline.
Late capsular block syndrome
Capsular block syndrome (CBS) is a complication of cataract surgery in which the capsular bag accumulates fluid between the IOL and the posterior capsule. This trapped fluid can cause distention of the posterior capsule and anterior displacement of the IOL. CBS occurs in less than 1% of cases and is classified as either early (occurring within the first few weeks following surgery) or late (months to years following surgery)[1]. One study found that axial eye lengths greater than 25 mm and patients that receive 4-haptic IOL compared to a C-loop IOL may have a higher prevalence of CBS [2]. Even rarer than CBS alone is CBS associated with Propionibacterium acnes infection within the capsular bag [3].
There are three categories of CBS: non-cellular, inflammatory, and fibrotic. In all subcategories, contact or adherence between the intraocular lens and the anterior capsule is the critical step that leads to fluid accumulation and subsequent capsular bag distension. Inflammatory and non-cellular CBS usually occur within the first week after cataract surgery. Fibrotic CBS occurs in the late postoperative period, months to years after surgery, and is typically due to lens epithelial cell proliferation and pseudo-metaplasia [2].
Patients will typically present with blurry vision due to a myopic shift from forward displacement of the IOL [2]. On exam, patients may have increased space between the optic and posterior capsule, anterior displacement of the iris-lens diaphragm leading to shallowing of the anterior chamber, elevated intraocular pressure and synechiae formation [1,2,4]. Potential complications of untreated CBS include: glaucoma, posterior capsule opacification, and posterior synechiae [4].
This case is unique as the patient started experiencing symptoms 10 years after cataract surgery. Most reported cases of late CBS have been observed within 5 years of surgery [4]. Therefore, it is important to keep CBS on the differential in any patient experiencing visual changes after cataract surgery, even when the surgery occurred many years prior.
AS-OCT can be used to evaluate the patient for CBS before and after YAG capsulotomy. Anterior chamber depth can be measured and anterior movement of lens-iris diaphragm can be observed with this technology when there is suspicion of CBS [5]. Additionally, as seen in Figure 1, AS-OCT can demonstrate collection of fluid between the lens and posterior capsule and its dissipation after YAG capsulotomy. Other imaging options include ultrasound biomicroscopy and the Scheimpflug camera. It has been shown that ultrasound biomicroscopy may be superior to Scheimpflug imaging when the capsular bag is extremely distended [6].
Capsular block syndrome is most commonly treated with Nd:YAG laser posterior and/or anterior capsulotomy [1,7]. This allows for release of the trapped fluid and return of the IOL and iris-lens diaphragm back to its intended position leading to resolution of myopic shift and improving visual acuity. Other potential treatments for CBS include: observation, use of anti-inflammatory medication drops in the presence of inflammation, surgical aspiration of the cortical masses and fluid, or pars plana vitrectomy with surgical removal of the posterior capsule [2,7]. P. acnes associated CBS should be treated with bimanual irrigation and aspiration behind the IOL to prevent spread posteriorly and reduce the risk of endophthalmitis [3].
Etiology
|
Signs
|
Symptoms
|
Treatment/Management
|
CBS is a rare complication of cataract surgery that can occur in the perioperative period or many years following the surgery. It is important to recognize and appropriately treat CBS in patients experiencing visual acuity changes with a history of cataract surgery, even if the surgery occurred many years prior.
Killoran E, Haugsdal J, Oetting TA. Capsular Block Syndrome: An Unusual Presentation. EyeRounds.org. July 6, 2016; Available from: https://eyerounds.org/cases/238-Capsular-Block-Syndrome.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
