
Chief Complaint: Red eyes for six weeks.
History of Present Illness: 23-year-old healthy white male presented with 6-week duration of red eyes associated with mild discharge, foreign body sensation, tearing, blurred vision, and swollen eye lids. These symptoms started in his right eye and, a few days later, his left eye also became affected. A week prior to his presentation, he was diagnosed at his local emergency department with conjunctivitis and was prescribed polymyxin B drops. However, his symptoms persisted and he decided to seek further medical attention.
Past Ocular History: Denies contact lens use, injury, surgery, or strabismus. Patient does wear corrective spectacles for mild myopia.
Medical History: None
Medications: Polymyxin B drops as noted. No allergies.
Family History: Non-contributory
Social History: The patient has had multiple female sexual partners in the past and uses barrier protection with intercourse most of the time. He denies drug or tobacco use. The patient consumes 3-4 alcoholic drinks per day on weekends and at parties.
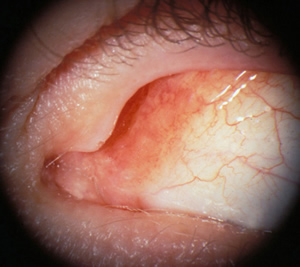
| 1A: Chronic follicular conjunctivitis in adult Chlamydial conjunctivitis. | 1B: Magnified view clearly shows the distinct follicles on the semilunar fold and bulbar conjunctiva. |
 |
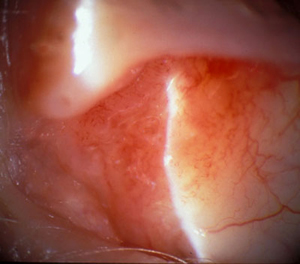 |
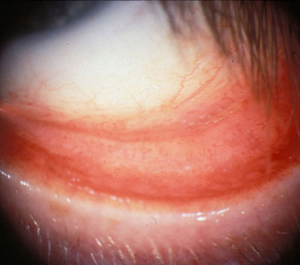
| 2A: Conjunctival injection, follicles, and chemosis were evident. | 2B: Magnified view of the palpebral conjunctiva. |
 |
 |
Course: Conjunctival scrapings were obtained and sent for culture. Growth of Chlamydia trochomatis resulted. The patient was started on oral doxycycline 100 mg BID for 1 month. After less than a week of systemic antibiotic therapy, his symptoms resolved completely.
The positive chlamydial culture alerted the Iowa Department of Public Health. The public health nurse reviewed the patient's sexual contacts for evaluation and treatment of sexually transmitted diseases.
Discussion: C. trachomatis, a human pathogen, is an obligate intracellular bacterium responsible for three different conjunctivitis syndromes: trachoma, adult and neonatal inclusion conjunctivitis, and lymphogranuloma venereum. The adult inclusion conjunctivitis is caused by serotypes D-K. C. trachomatis is the most common cause of chronic follicular conjunctivitis and is also responsible for 20% of acute conjunctivitis cases (Fitch et al. 1989).
Chlamydial conjunctivitis is a sexually transmitted disease and occurs most commonly in sexually active young adults. Women are more susceptible than men. The disease is usually transmitted through hand-to-eye spread of infected genital secretions. The incubation period is one to two weeks.
Patients can present with a wide range of acuity and severity of symptoms. Some present with acute, mucopurulent conjunctivitis but more commonly patients have mild symptoms for weeks to months. Chlamydial conjunctivitis is often a unilateral disease but can involve both eyes. Patients complain of pink/red eye, mucous discharge, crusting of lashes, lids stuck together, swollen lids, tearing, photophobia, foreign body sensation, and decreased vision. Close questioning may reveal genitourinary symptoms, particularly among women. The sexual partners of these patients may have similar symptoms. Because the presenting symptoms of chlamydial conjunctivitis mimic those of viral and other bacterial (e.g. staphylococci) conjunctivitis, many of these patients may have been previously treated with topical antibiotics without symptomatic relief.
The clinical findings seen in chlamydial conjunctivitis may also resemble other forms of infectious conjunctivitis. On clinical examination, patients may have palpable lymphadenopathy, particularly involving the preauricular nodes. Anterior segment examination often reveals mucous discharge, conjunctival hyperemia, and chemosis. Follicular reaction is a key feature of chlamydial conjunctivitis and typically involves the bulbar conjunctiva and semilunar folds. The cornea may exhibit both fine and coarse epithelial and subepithelial infiltrates. Occasionally, micropannus may develop on the superior cornea. Conjunctival scarring is rarely seen in developed countries because of prompt treatment.
A diagnosis is made based on signs, symptoms, and clinical suspicion. The preferred confirmatory test is to culture the organism. Giemsa staining has been the only method available to detect chlamydia for about 50 years. The classic finding is the basophilic intracytoplasmic inclusions. More recently, direct immunofluorescent staining (DFA), culture, and enzyme-linked immunosorbent assay (ELISA) have been developed for detection of chlamydial infection.
If left untreated, adult chlamydial conjunctivitis resolves spontaneously in 6-18 months. Chlamydial conjunctivitis can be treated topically with tetracycline, erythromycin, and fluoroquinolones. However, due to the high prevalence of concomitant genital tract infection, systemic antibiotic therapy is recommended. Though there is some variation in recommendations between sources, accepted treatment options include: azithromycin 1000mg single dose, doxycycline 100mg BID for 7-10 days (Sutphin JE, 2004), tetracycline 100mg QID for 7-10 days, or erythromycin 500mg QID for 7 days. Recently, an open, randomized clinical trial showed that azithromycin 1000mg single dose was equally efficacious when compared to doxycycline 100mg BID for 10 days in eradicating C. trachomatis and acheiving clinical cure (Katusic et al. 2003).
Because adult chlamydial conjunctivitis is a sexually transmitted disease, co-infection needs to be considered. The most common co-infection is gonorrhea. A common practice is to administer single dose therapy for both chlamydia and gonorrhea infections. Sexual partners of the patients should be contacted, and they should be evaluated and treated for STD.
EPIDEMIOLOGY
|
SIGNS
Histopathology: basophilic intracytoplasmic epithelial inclusion bodies (on Giemsa staining) |
SYMPTOMS
|
TREATMENTOptions include one of the following:
|
Yang EB, Oetting TA: Adult Chlamydial Conjunctivitis: 23-year-old male with 6-week duration of red eyes. EyeRounds.org. February 28, 2007; Available from: http://www.EyeRounds.org/cases/68-Adult-Chlamydial-Conjunctivitis-Red-Eyes-Chronic.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
