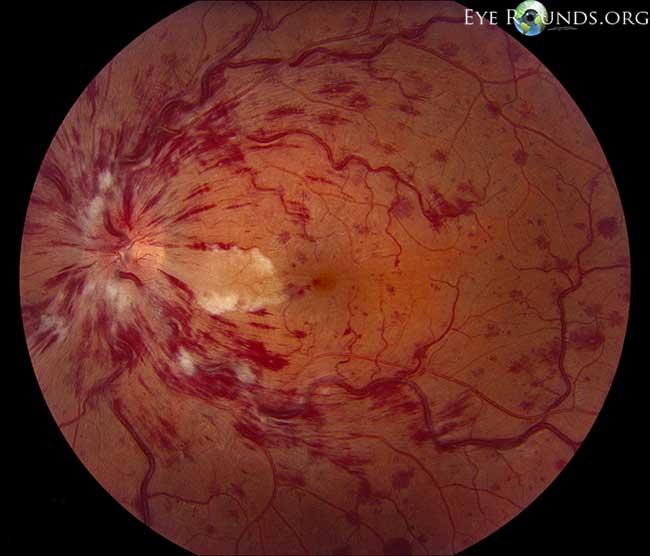
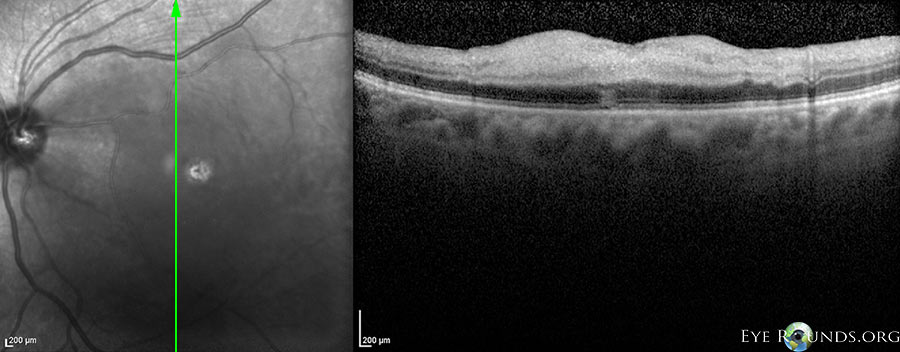
A 67-year-old man with history of type 2 diabetes mellitus, hyperlipidemia, and uncontrolled hypertension presented with a central visual field deficit of sudden onset in his right eye. Visual acuity on presentation was 20/25 in both eyes, and funduscopic examination revealed an isolated cilioretinal artery occlusion (CLRAO) in his right eye (Figure 1). Work-up revealed significant right internal carotid artery stenosis (>50%). A right carotid endarterectomy was performed, and vascular risk factors were optimized. Visual acuity was stable at 20/25 one month after presentation.
CLRAO accounts for ~5-7% of retinal artery occlusions and is usually associated with a central retinal vein occlusion (CRVO) or anterior ischemic optic neuropathy (AION). [1-3] Less commonly, CLRAOs may occur as an isolated phenomenon as in this case. Isolated CLRAOs typically have a better visual prognosis than those associated with a CRVO or AION with 90% of patients achieving a visual acuity of 20/40 or better. [3]




Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links