
Chief Complaint: Referral for evaluation of glaucoma
History of Present Illness: A healthy 47-year-old female with no family history of glaucoma was referred for possible glaucoma. She denied any visual complaints.
Past Ocular History: Hyperopia and presbyopia
Medical History: Iron deficiency anemia secondary to uterine fibroid
Visual acuity with correction
MRx
Pupils: symmetric, briskly reactive and there is no relative afferent pupillary defect OU
Visual Fields: full by confrontation OU
Intraocular Pressure by Applanation Tonometry
Anterior Segment Examination:
Conjunctiva: normal
Cornea: clear without Kruckenberg spindle or endothelial changes
Iris: normal architecture without heterochromia or transillumination defects
Anterior chamber: narrow angles by Van Herrick
Lens: Clear OU
Gonioscopy (Spaeth classification):
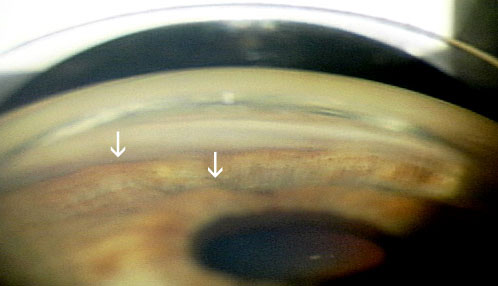 |
Video: first note the anterior chamber is shallow by Van Herrick. On indentation gonioscopy, the "double hump" is observed |
 |
 |
 |
This patient was initially treated with LPIs in each eye. Her angle depth improved in each eye but there was concern that the angle in the left eye was still occludable. She underwent a laser iridoplasty OS without complication and repeat gonioscopy demonstrated improvement in the angle depth OS. At present, the angle in the right eye does not appear to be occludable and we are monitoring her with repeat gonioscopy exams every 6 months.
Plateau iris syndrome is a relatively uncommon form of primary angle closure glaucoma that is seen more often in younger adults than pupillary block angle-closure glaucoma. It is caused by large or anteriorly positioned ciliary processes that push the peripheral iris forward. The mechanical position of the ciliary processes against the trabecular meshwork crowds the angle and obstructs aqueous outflow. A component of pupillary block is often present.
The central anterior chamber may appear to be of normal depth on slit lamp examination. On examination with gonioscopy, the iridocorneal angle is usually crowded or even closed. The iris typically appears to have a flat approach (on a plane to intersect Schwalbe's line) with a steep drop-off just before the trabecular meshwork. On indentation gonioscopy the "sine wave" or "double-hump sign" is seen. The peripheral "hump" is created by the iris draping over the ciliary body and the more central hump by the iris curving over the anterior lens surface.
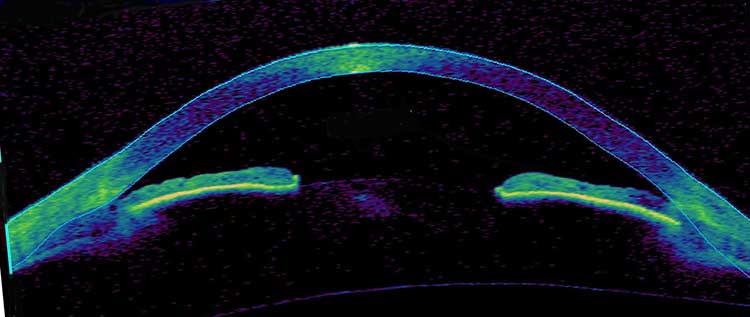
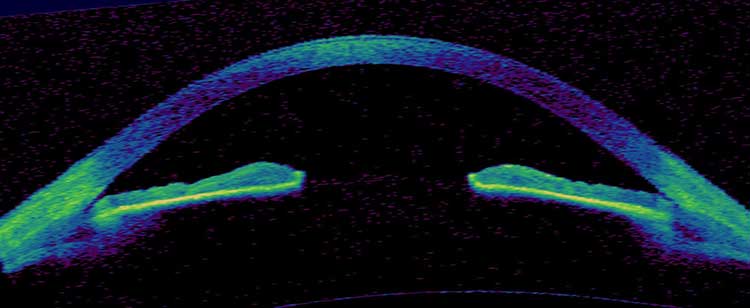
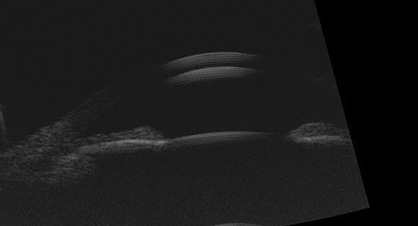
Ancillary imaging modalities can be helpful in making the diagnosis of plateau iris. Ultrasound biomicroscopy can provide information of the anterior segment anatomy as well as help confirm any element of pupillary block. Anterior segment optical coherence tomography (OCT) can also provide insight into the anatomy, but it is not a dynamic examination and does not provide as much information as gonioscopy.
Some element of pupillary block frequently exists in patients with plateau iris configuration and generally, peripheral laser iridotomy should be performed as the first intervention in patients suspected of having plateau iris. This often times is an adequate treatment for eyes with plateau iris configuration. However a subset of patients will have a persistent occludable angle despite a patent iridotomy causing plateau iris syndrome. Eyes where the iridocorneal angle has persistent apposition or the intraocular pressure remains elevated should be treated with laser iridoplasty. The goal of laser iridoplasty is to place laser burns at the peripheral iris to shrink the iris and pull it from the angle. Of course, if laser surgical treatment is ineffective in controlling the intraocular pressure, conventional surgical procedures such as a trabeculectomy or a tube-shunt may need to be implemented.
Laser settings recommended by Wallace L.M. Alward, MD in Glaucoma: The Requisites in Ophthalmology.
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
| TREATMENT
|
Additional Resources available at www.gonioscopy.org
References
Rogers GM, Alward, WLM, Fingert JH. Plateau Iris. EyeRounds.org. December 21, 2011; Available from: https://eyerounds.org/cases/143-plateau-iris.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
