
"My vision is blurry and I have a headache."
A 17-year-old boy presented with blurry vision in both eyes. He reported that his blurry vision started several months prior. He denied focal visual loss in either eye. He also reported headaches starting around the same time as his blurred vision. He had no prior history of headaches. The headaches were present almost every day and were interfering with his ability to perform well in school. He denied associated nausea or vomiting. He denied any diplopia, transient visual obscurations (TVOs), pulse-synchronous tinnitus (PST), recent weight gain, or snoring while sleeping. Several weeks prior to the onset of his headaches and blurred vision, he had started somatropin (Norditropin Flexpro) injections, which were prescribed by his endocrinologist for short stature in the setting of growth hormone deficiency. He had no fevers, chills, night sweats, or focal neurological symptoms.
Fundus Photography was obtained at initial presentation and is shown in Figure 1.
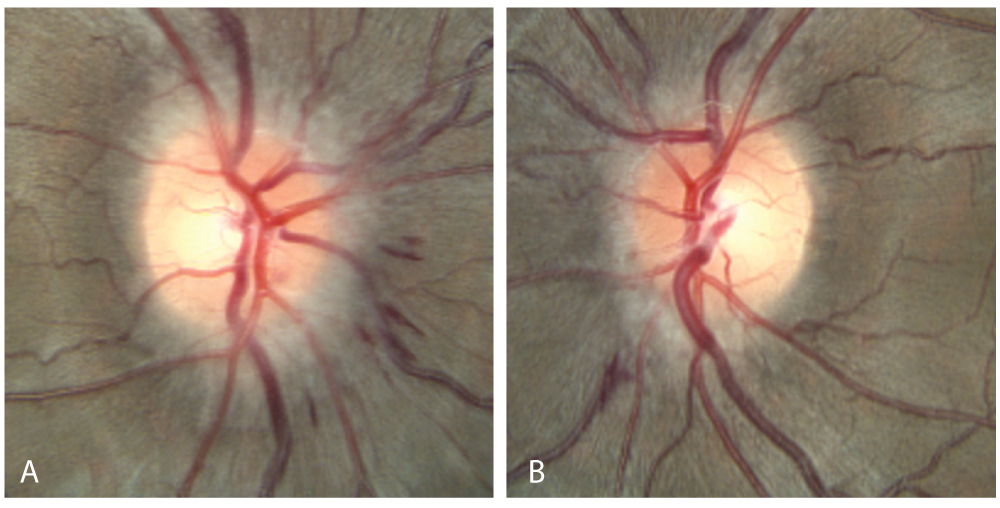
Figure 1: Fundus photography of the right eye (A) and the left eye (B) showing Grade 1 disc edema of both optic nerves characterized by a "C-shaped" halo with associated disc hemorrhages. There was no optic disc pallor in either eye. There were no peripapillary folds or coarsening of the retinal nerve fiber layer (RNFL) in either eye.
The differential diagnosis for papilledema is broad. Below is a brief differential diagnosis. For a more comprehensive review, please view the following link: (https://eyerounds.org/cases/99-Pseudotumor-Cerebri.htm).
An extensive workup was ordered to rule out intracranial pathology. Kinetic (Goldmann) perimetry was obtained and was normal except for mildly enlarged blind spots. Optical coherence tomography (OCT) of the optic nerve head revealed thickening of the retinal nerve fiber layer (RNFL) consistent with optic nerve edema. OCT of the ganglion cell layer (GCL) was normal without signs of atrophy. B-Scan ocular ultrasonography was negative for disc drusen. Magnetic resonance imaging (MRI) and magnetic resonance venography (MRV) of the brain were obtained prior to presentation; these were reviewed and showed globe flattening, an empty sella, and sagittal sinus narrowing without concern for thrombosis. He was later scheduled for a lumbar puncture, which was significant for an opening pressure of 19 cm H2O with normal constituents.
He was diagnosed with growth hormone-related idiopathic intracranial hypertension and it was recommended that his somatropin dose be reduced. His endocrinologist tapered from 2.9 mg to 2.0 mg six times weekly. He was started on oral acetazolamide 250 mg twice daily and titrated up to 500 mg twice daily. He was also encouraged to lose 5-10% of his body weight. At 3 months follow up, his headaches and blurry vision had fully resolved and he was visually asymptomatic. His visual fields were full and his disc edema had mostly resolved with trace residual edema of both optic nerves as shown in Figure 2.
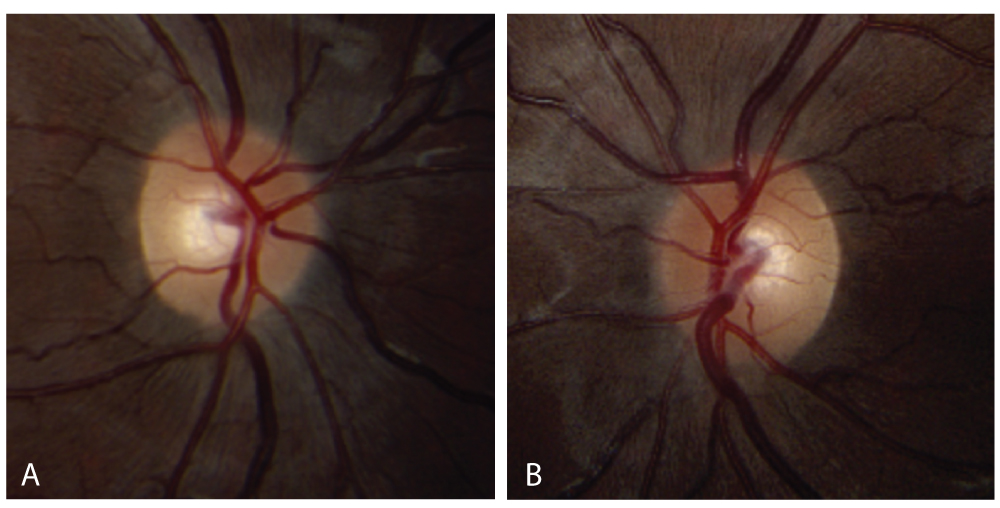
Figure 2: Fundus photography of the right eye (A) and left eye (B) at final presentation showing trace disc edema of both optic nerves following treatment. There were no peripapillary folds or coarsening of the retinal nerve fiber layer (RNFL).
Intracranial hypertension (IH) is characterized by increased intracranial pressure (ICP) that can result in swelling of the optic nerves and subsequent vision loss. This disorder may be caused by a variety of underlying conditions and requires a thoughtful clinical, laboratory, and radiological workup. Recent studies have shown growth hormone (GH) therapy in patients with growth hormone deficiency (GHD) to be a rare, but significant cause of IH [1 ,2].
Intracranial hypertension (IH) is now a well-established adverse effect associated with GH therapy [3]. Although the exact incidence is unknown, IH occurs in approximately 1.2 per 1000 children on hormone therapy [4]. Important risk factors include obesity as well as aggressive GH therapy, including high dosage and rapid escalation of treatment [1]. In the literature there is not a specific dosage of GH reported that definitively causes IH, but many studies show improvement of IH with reduction of GH therapy [2]. The incidence of this disease is increased in patients with renal failure or chromosomal abnormalities such as Turner syndrome and Prader-Willi syndrome [1]. There does not appear to be a sex predilection in patients with IH caused by GH therapy [5]. Malozowski et al studied a cohort of 13 patients and found the mean age of affected patients to be 9 with a range of 3 to 16 years old [2].
GH is an anabolic hormone synthesized by the anterior pituitary gland. Its production is under tight regulation via peptides secreted by the hypothalamus, liver, and stomach as shown in Figure 3. GH facilitates somatic growth and plays a critical role in protein, lipid, and carbohydrate metabolism [6].
GHD is a medical condition characterized by inadequate production and/or secretion of GH by the pituitary gland, which results in dwarfism or growth retardation. GHD is often treated with GH therapy. Although the pathogenesis of IH in patients with GHD treated with GH therapy is not fully understood, it is thought that GH increases IGF-1-mediated production of cerebral spinal fluid (CSF) from the choroidal plexus, leading to increased intracranial pressure [3].
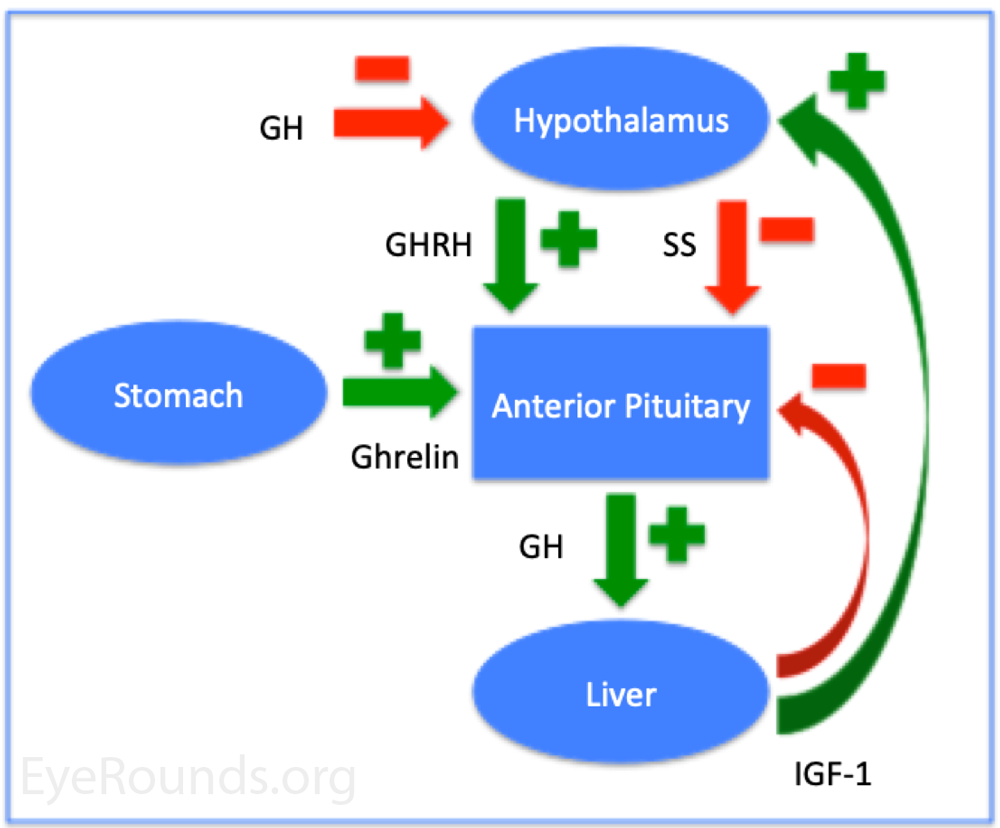
Figure 3: Diagram depicting the control of growth hormone. The color green indicates positive feedback loops; the color red indicates negative feedback loops. Abbreviations: Growth hormone (GH), growth hormone releasing hormone (GHRH), somatostatin (SS), insulin growth factor-1 (IGF-1).
The most common presenting complaint by children with IH due to GH therapy is intractable headache [7]. The headaches are often associated with nausea and vomiting, and are often positional being worse with lying down. Although uncommon, some patients present without headache [8]. Visual symptoms are common in this condition and patients may report bilateral blurry vision and transient visual obscurations (TVOs) as well as pulse synchronous tinnitus (PST) [7]. PST is often described as a "whooshing" sound in the ears synchronized with their pulse. Diplopia may occur from an associated sixth nerve palsy and is often described as a horizontal diplopia that is worse with lateral gaze [7]. It is not uncommon for patients with IH on GH therapy to be asymptomatic [9]. Prior research suggests that the onset of symptoms usually occurs within weeks to months after starting GH replacement but may rarely occur years later [2].
Ophthalmic signs can include decreased visual acuity, strabismus consistent with a sixth nerve palsy, a relative afferent pupillary defect with asymmetric disease, and visual field defects including enlarged blind spots. Fundus examination reveals optic nerve head disc edema that may be associated with disc hemorrhages, peripapillary folds, and/or coarsening of the RNFL. OCT of the optic nerve heads and ganglion cell layers are important measures of nerve fiber layer swelling and subsequent atrophy. B-scan ultrasonography may be utilized in atypical cases to rule out disc drusen as a source of pseudopapilledema. If papilledema is suspected, lumbar puncture with opening pressure and MRI/MRV of the brain are necessary to rule out intracranial pathology.
The cornerstone of treatment involves close collaboration with the patient's endocrinologist and cessation or reduction of GH therapy if medically appropriate [2]. This may be sufficient for patients who are relatively asymptomatic and who do not have vision-threatening disease. In general, weight loss of about 5-10% of body weight is encouraged in obese patients. Medical treatment is considered in patients with severe papilledema and may include acetazolamide, topiramate, furosemide, and/or thiazide diuretics. For a more comprehensive discussion of treatment options in IH view the following link (https://webeye.ophth.uiowa.edu/eyeforum/article/IIH/pc-medical-tx.htm).
Prognosis is usually good with the majority of patients having resolution of papilledema with treatment and stopping/reducing GH replacement therapy [2]. The course is usually benign without long-term vision loss. Persistent IIH is less common [2]. It is important to recognize that patients who are restarted on GH therapy may redevelop papilledema [2].
ETIOLOGY/PATHOPHYSIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Quist TS, Wall M. Growth hormone-related intracranial hypertension. EyeRounds.org. October 30, 2019; Available from: https://eyerounds.org/cases/288-gh-related-iih.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
