
Blurred vision of the right eye with constriction of visual field
A 61-year-old woman presented for evaluation of sudden onset blurry vision of the right eye, with associated complete loss of the right inferior visual field. The patient stated that the sudden vision loss occurred while she was taking a shower. She could not recall any preceding events leading up to the acute vision loss or any similar events in the past. She denied difficulty walking or standing; however, her husband stated that she appeared unsteady while walking. She denied headaches, neck pain, weakness, or numbness. She initially presented to her local emergency room where she was first evaluated by neurology and emergently worked-up for a possible stroke. CT angiogram of the head and brain revealed findings concerning for a right vertebral artery obstruction and she was transferred to the University of Iowa Hospitals and Clinics (UIHC) for further evaluation. Upon arrival to UIHC, the patient underwent an MRA of the head and neck with and without contrast, which demonstrated 70% stenosis of the right internal carotid, and less than 50% stenosis of the left internal carotid. Given the presence of reported right inferior hemianopia with significant carotid stenosis, evaluation by ophthalmology was requested.
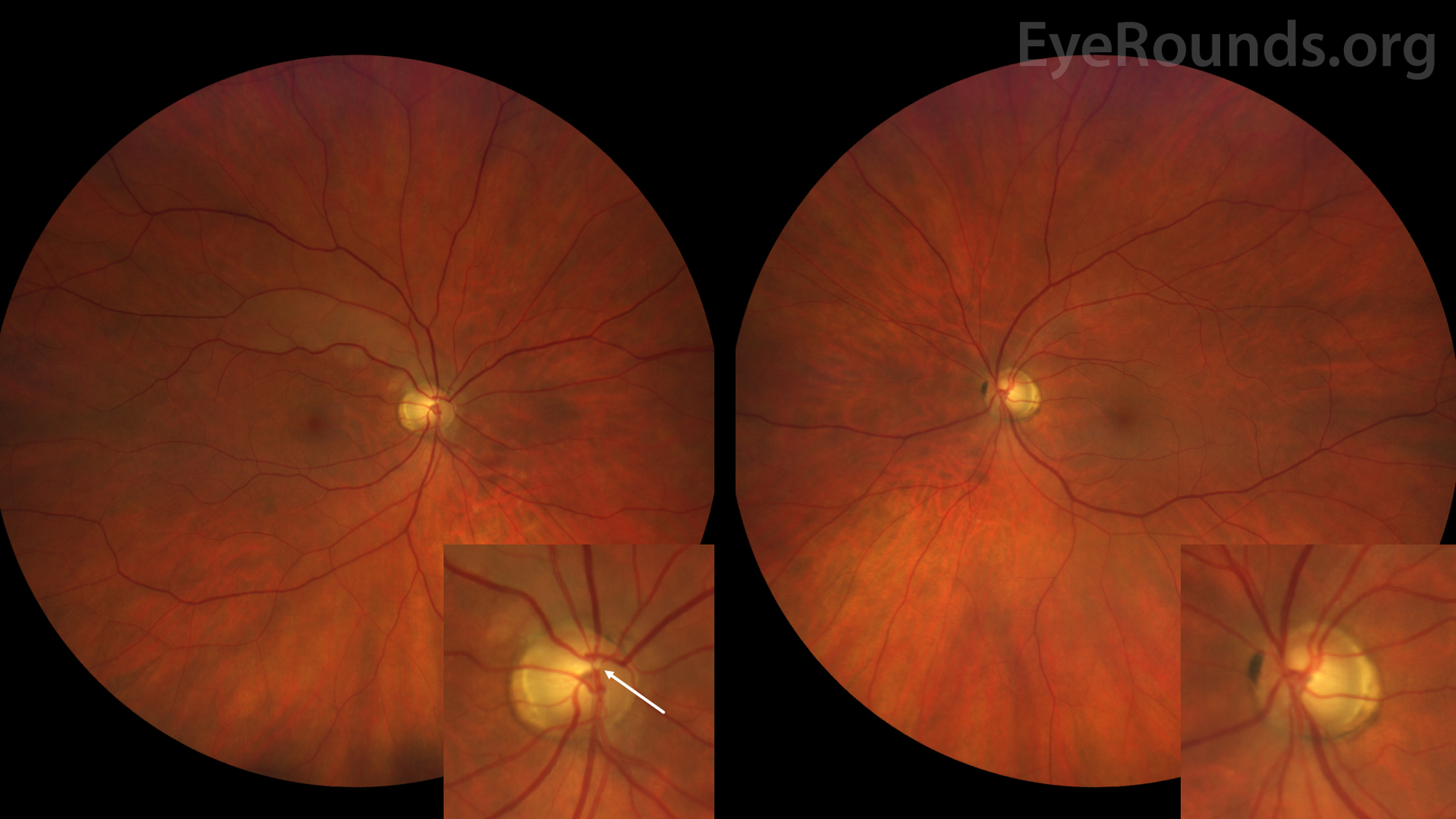
Figure 1: Color fundus photography of the right eye (left panel) demonstrates a large cup-to-disc ratio of 0.6 with associated peripapillary atrophy and a Hollenhorst plaque lodged within a branch point of the superior arcade. Diffuse retinal whitening can be seen extending along the superior arcade. The Hollenhorst plaque is better appreciated in the inset. Color fundus photography of the left eye (right side image) demonstrates a symmetric enlarged cup-to-disc ratio of 0.6 and peripapillary atrophy. No embolus of the left eye is identified.
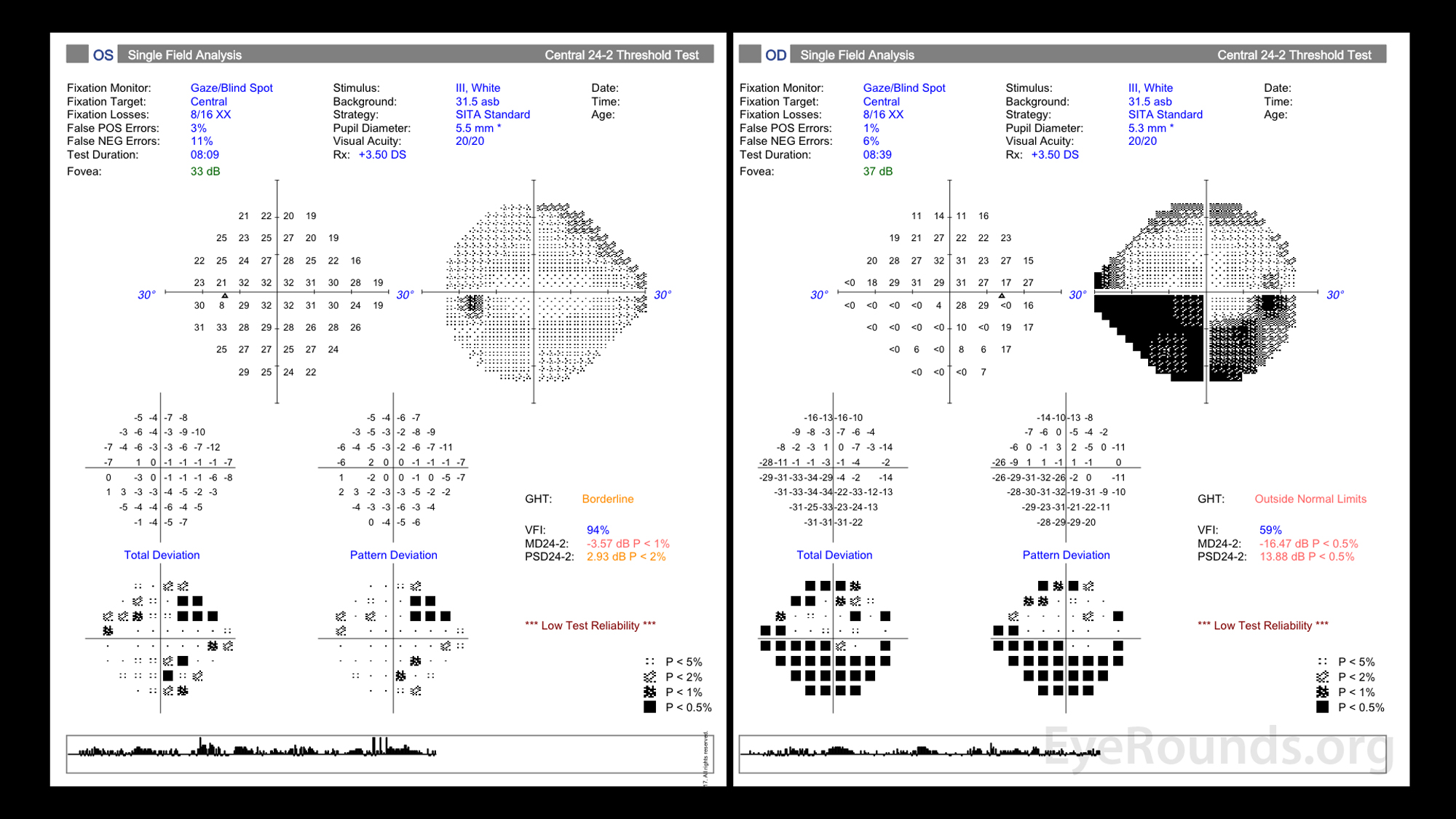
Figure 2: Visual field testing in both eyes demonstrated poor testing reliability. The right eye visual field (right panel) demonstrates an inferior defect that extends in an arcuate pattern originating from the optic disc. The defect is greatest nasally and respects the horizontal meridian. The left eye (left panel) demonstrates non-specific changes.
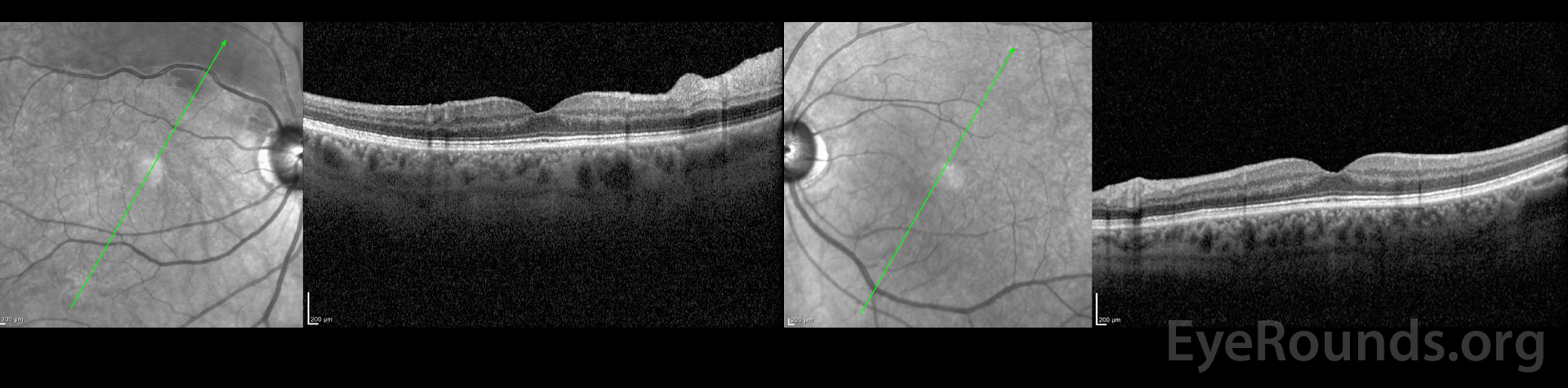
Figure 3: OCT of the right eye (left panel) is significant for diffuse inner retinal thickening extending along the superior arcade. The macula is otherwise normal. OCT of the left eye (right panel) is normal.
Branch retinal artery occlusion of the right eye
No acute ophthalmic intervention was initiated because symptom onset occurred >18 hours prior to evaluation. The patient was started on aspirin 81mg, clopidogrel, and atorvastatin therapy for the secondary prevention of stroke. Though clopidogrel was recommended, the patient voiced concerned about the bleeding risk associated with dual anti-platelet therapy and was only intermittently compliant before ultimately self-discontinuing. She was evaluated by interventional neurology who recommend the patient be scheduled for a stent assisted angioplasty.
Retinal artery occlusion occurs when an artery in the retina is blocked, most commonly due to emboli. Occlusion of the central retinal artery (CRAO), a branch of the central retinal artery (BRAO), or the cilioretinal artery (CLRAO) may occur. The sensitive neural tissue of the retina is highly dependent on adequate blood flow; therefore occlusion of one of these arteries can have profound visual effects resulting in transiet or permanent visual field loss [1, 2].
CRAO and BRAO are rare entities. The incidence of CRAO is between 1-2 persons per 100,000 per year [3] while the incidence of BRAO is closer to 5 per 100,000 persons per year [2]. Retinal artery occlusion can occur in patients of all ages, but is more common in older adults. Some causes, such as thrombophilia, are more often seen in younger adults [4, 5].
Risk factors for embolic BRAOs are similar to risk factors for cardiovascular disease. Diabetes mellitus, hyperlipidemia, hypertension, coronary artery disease, tobacco use, history of cerebral vascular accidents, and family history of vascular disease all pose significant risk in the development of CRAO and/or BRAO. Less common risk factors include: sickle cell disease, myeloproliferative disorders, antiphospholipid antibody syndrome, hypercoagulable states, IV drug use, and oral contraceptive use [4, 5].
The central retinal artery and/or the cilioretinal artery (present in 20-25% of eyes) supply the retina. The internal carotid artery gives rise to the central retinal artery which branch at the optic nerve head into the superior and inferior arcades while the cilioretinal artery originates from the posterior ciliary artery.
BRAO results in decreased perfusion to the retina resulting in retinal ischemia, which leads to necrosis of the inner layers of the retina and consequent loss of vision [6]. The severity of retinal damage is associated with elapsed time of occlusion and the area of retina affected. Primate studies have shown that irreversible damage occurs after 4 hours, but may occur in as little as 90 minutes [7].
Carotid artery plaques are the most common source of emboli. Such plaques are derived from cholesterol (Hollenhorst plaques). Platelet-fibrin emboli and calcific cardiogenic emboli are also common sources. More rare entities such as fat emboli, septic emboli originating from diseased heart valves, and atherosclerotic emboli dislodged during vascular procedures can also cause BRAO [4, 8].
BRAO may be associated with other conditions affecting the carotid, ophthalmic, or retinal arteries. Some of these entities include: Crohn's disease, Lyme disease, multifocal retinitis, Meniere's disease, migraine, prepapillary loops, Susac syndrome, toxoplasma chorioretinitis, sickle cell disease, Takayasu arteritis, Whipple disease, and others. It may also be caused by states of relative hypoperfusion either from increased intraocular pressure or decreased perfusion during a vasospastic event. It is important to note that while GCA can cause CRAO and/or CLRAO (cilioretinal artery occlusion), GCA cannot cause BRAO since GCA affects larger vessels. These "branch retinal arteries" are technically smaller arterioles [4].
Patients commonly present with sudden painless monocular vision loss. The degree of vision loss depends upon the vessel implicated. BRAO typically results in much less severe visual loss than CRAO and is usually restricted to a section of the visual field. In more than half of BRAO cases, visual acuity is not drastically impaired [9]. Seventy-four percent of patients with a permanent BRAO and ninety-four percent of patients with transient BRAO present with 20/40 vision or better. In contrast, seventy-four percent of patients with CRAO present with vision worse than CF [1].
Fundoscopic exam of the affected eye may acutely demonstrate cotton wool spots. Within hours to days, retinal opacification (whitening) along the section of the blocked artery will appear. Often an embolism at the site of occlusion is visualized during fundoscopic exam [10]. It is important to also assess the contralateral eye for evidence of small vessel disease, and to probe patients for additional history if GCA is on the differential.
Only limited evidence exists regarding the efficacy of immediate treatment of embolic retinal artery occlusion. Some methods include: ocular massage, Nd:YAG laser, IOP-lowering medications, hyperventilation, and hyperbaric oxygen; however, none have strong evidence of improving visual outcomes [12]. Thrombolytic therapy has been investigated but is controversial [11]. Most importantly, symptomatic carotid artery disease can be treated with medical therapy or endarterectomy in patients with more than 70% carotid artery occlusion. Secondary prevention therapies are important for strokes or TIA, such as antiplatelet therapy, statin therapy, or thromboembolic prophylaxis.
Complications of both CRAO and BRAO include neovascularization. In a retrospective review of 286 eyes (83 CRAOs and 203 BRAOs), 14.5% of CRAO eyes developed neovascularization. Of these, iris neovascularization predominates with neovascular glaucoma developed in 83% of eyes. In contrast, iris neovascularization occurred in <1% of BRAO eyes [13]. Intravitreal anti-vascular endothelial growth factor (anti-VEGF) and panretinal photocoagulation are reserved for neovascular complications [11].
According to the Centers for Disease Control and Prevention, stroke is a major cause of serious long-term disability and the fifth leading cause of death in the United States. While most healthcare providers are trained to recognize the presenting signs and symptoms of a stroke, few may recognize a CRAO or BRAO, which are considered stroke equivalents, as an indication for prompt stroke work-up at a certified stroke center.[11] Despite the National Stroke Association, American Heart Association, and American Academy of Ophthalmology guidelines recommending referral of such patients, only 18-35% of ophthalmologists report referring patients presenting acutely for an embolic retinal artery occlusion [12].
The primary role of the ophthalmologist is to first identify and recognize a CRAO or symptomatic BRAO, and then refer to a stroke center for additional work-up. In patients older than 50 years of age, GCA should also be considered. If there is a high clinical suspicion for a suspected arteritic process such as GCA, immediate treatment with high dose systemic corticosteroids should be initiated. Non-acute or asymptomatic BRAO still merit systemic work-up, but there is limited evidence for urgent stroke center referral [11].
It is important to recognize that symptomatic patients may not always present to an ophthalmologist office; therefore, all primary care providers (particularly emergency department physicians and trainees) be aware of the preferred practice patterns set forth by the American Academy of Ophthalmology in the management of acute symptomatic retinal and ophthalmic artery occlusions. Emergency department physicians and trainees should also be familiar with these guidelines should there be no stroke center available for prompt referral. A quick resource guide to find the nearest stroke center is: https://www.npr.org/2009/12/11/121051484/find-a-certified-u-s-stroke-center-near-you.
A typical stroke work-up may include: MRA of the head and neck, evaluation of the carotid arteries via Doppler ultrasound or CTA, EKG, echocardiogram, and blood pressure and cardiac monitoring [12]. In patients 50 years or younger, workup may also include specialized coagulation studies (e.g., protein C&S, factor V Leiden, anticardiolipin, and lupus anticoagulant). Vasculitides, myeloproliferative, or sickle cell disease should also be considered [11].
In addition to the above evaluation, ophthalmologists also have a supportive role to play in primary prevention. Ophthalmologists should work closely with a patient's primary care physician to ensure all modifiable risk factors such as: hypertension, atherosclerotic disease, coronary artery disease, diabetes, and smoking are being addressed properly.
Fifteen to twenty-five percent of patients with acute retinal ischemia also have evidence of stroke and/or have a significant risk of stroke, even if presenting without other focal neurologic deficits.[12] Eighty percent of patients with CRAO suffer visual acuities 20/400 or worse while more than 90% of patients with BRAO will see better than 20/40.[8] Improvement usually occurs within weeks.
EPIDEMIOLOGY/ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT[11]
|
Diel RJ, Mortensen Z, Folk JC, Johnson AT. Symptomatic Branch Retinal Artery Occlusion: An Under-Recognized Sign of Stroke. EyeRounds.org. Posted April 14, 2020; Available from https://EyeRounds.org/cases/293-symptomatic-BRAO.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
