Chief Complaint: 11-year-old male seen for evaluation of an open globe and traumatic cataract.
History of Present Illness: An 11-year-old male was referred to the University of Iowa Hospitals and Clinics for evaluation of a possible open globe. One day prior, while hammering on a taillight of an old automobile a glass shard flew into his right eye. The boy complained of pain and a foreign body sensation and was taken to the local emergency treatment center for evaluation. A slit lamp examination failed to reveal a foreign body. Early the next morning he awoke with worsening pain and decreased vision. A local ophthalmologist noted a corneal laceration and cataract, but could not rule out the presence of an intraocular foreign body and referred him to the UIHC.
Upon arrival, he continued to complain of pain and decreased vision in his right eye.
Past Ocular History: No prior ocular injury, surgery, or illness.
Past Medical History: Non-contributory
Medications: Gatifloxacin (Zymar) ophthalmic drops, 4x/day, in the right eye.
Family and Social History: Noncontributory
Other examination: No IOFB detected by maxillofacial CT or ocular echography. The posterior lens capsule appeared to be intact with b-scan echography.
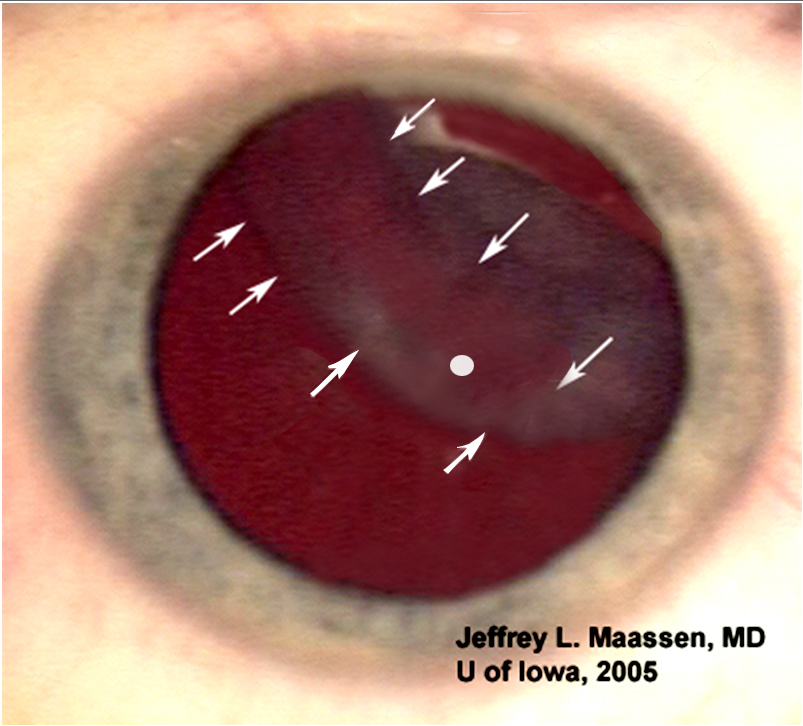
Discussion: This case presents the interesting challenge of dealing with a traumatic cataract with anterior capsular rupture. When considering our surgical approach to this case, the most important consideration was identifying the anterior capsule. The anterior capsule appeared to be torn in a linear fashion from the 11:00 to the 4:00 position; however, protruding cortical lens material obscured the defect making it difficult to see the extent and position of the tear.
Poor visualization of the anterior capsular edges hampers initiating a capsulorhexis. Even if an adequate capsulorhexis opening were achieved, aspiration of the lens material would be difficult due to poor visualization and possible aspiration of the remaining anterior capsule. To aid in identifying the capsule, we elected to use a capsular stain.
Indocyanine green (ICG) was initially described for use as a capsular stain in mature cataracts by Horiguchi, et al (Horiguchi, et al 1998). After comparing the results of ten mature cataracts operations assisted by ICG stain they concluded it was safe and effective.
Trypan blue was described by Melles, et al (Melles, et al 1999) as a safe and an effective anterior capsular stain in mature cataracts. A recent study by Chung, et al (Chung, et al 2005) further established that ICG 0.5% and trypan blue 1% were safe in regards to endothelial cell count, corneal clarity, intraocular inflammation, and postoperative intraocular pressure.
The use of ICG in traumatic cataract was initially described in a case report by Newsom and Oetting (2000). In their case they demonstrated that ICG showed preferential staining of the capsule over the lens material. Identification of ICG stained lens capsule and facilitated completion of the capsulorhexis.
Trypan stained anterior capsule visualization in traumatic cataract was subsequently reported by Baykara, et al (Baykara, et al 2002).
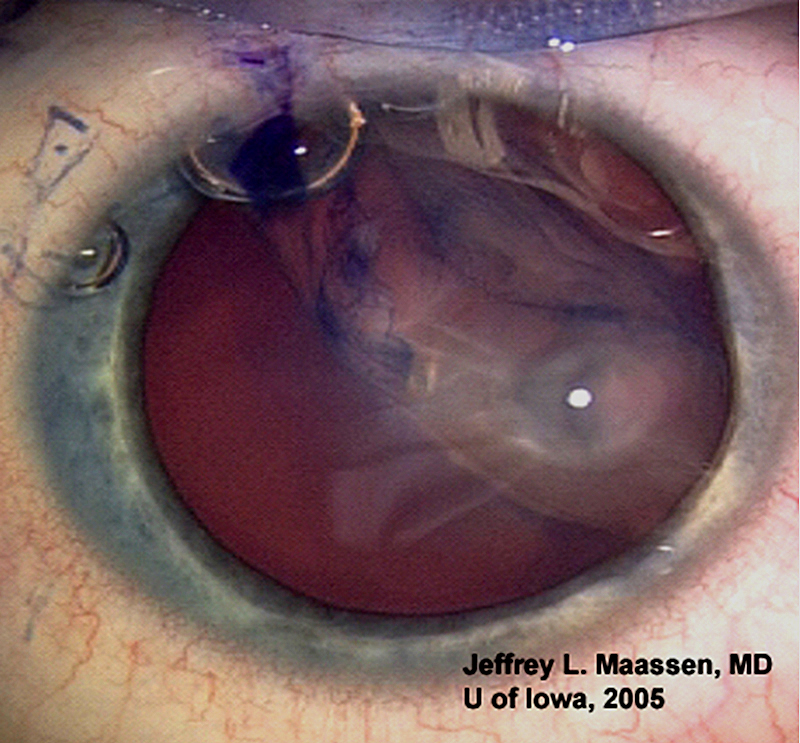
Description of Operative Procedure and Patient Course: Two days after the injury, cataract extraction was performed. A single paracentesis port was placed at the ten o’clock position. A bubble of filtered air was injected through the paracentesis until the anterior chamber was full. A commercial preparation of 1% trypan blue was injected under the bubble by injection of Viscoat and evacuation of air and trypan blue from anterior chamber. (Figure 2). The anterior capsule stained blue, but the anterior cortical material did not stain. A 2.7 mm incision into the anterior chamber followed by a cystotome to create a nick in the temporal portion of the anterior capsule. A continuous curvilinear capsulorhexis was performed with Utrata forceps. The cortical and nuclear portions of the lens were removed by irrigation/aspiration.
A foldable acrylic lens was injected into the intact capsular bag and the remaining viscoelastic was aspirated. The corneal laceration was sutured with two 10-0 nylon sutures. The wound was closed with 10-0 Vicryl suture.
Postoperative day #1 the patient was 20/70, the corneal laceration was Seidel negative, but there was a small piece of residual cortical material centered near the pupil. No residual corneal or capsular staining was noted. Postoperative day #2 his vision was 20/40 and the lens remnant was gone. Postoperative week #1 his vision was 20/30+.
Conclusion: This case further supports the earlier finding of Newsom and Oetting (2000) that capsular stains have greater affinity for the anterior capsule than for lens material. In this setting, trypan blue offers several advantages for traumatic cataract removal.
A recent letter to the Journal of Cataract and Refractive Surgery (Bishop, 2005) suggests that any type of capsule staining technique is contraindicated once the anterior capsule has been opened. We strongly disagree with this assertion. We propose the opposite and suggest that the preferred technique for initiating the capsulorhexis in cases of traumatic anterior capsular tear is the initial use of capsular stains such as ICG and trypan blue.
Diagnosis: Self-sealing corneal laceration with traumatic cataract and anterior capsular rupture
Maassen JL, Oetting TA, Johnson AT: Traumatic Cataract: 11-year-old boy with glass injury to the right eye. Eyerounds.org. February 16, 2006; Available from: http://www.EyeRounds.org/cases/51-Traumatic-Cataract-Eye-Injury-Capsular-Stain.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links