
Chief Complaint: 12-year-old boy with gradual progressive ptosis OU.
History of Present Illness: His parents noted painless, progressive, constant ptosis over the last 3 years. The patient denied symptoms of diplopia, weakness, or speech/swallow troubles. He was healthy as a young child.
PMH/FH/POH: NSVD. Healthy. No POH. FH negative for history of ptosis/diplopia. No neurologic disease. Two sisters age 6 who are healthy.
| OD | OS | |
|---|---|---|
| Palpebral fissure (PF) | 5 mm | 3 mm |
| Margin reflex distance 1 (MRD1) | 0 mm | -2 mm |
| Margin reflex distance 2 (MRD2) | 5 mm | 3 mm |
| Levator function (LF) | 8 mm | 8 mm |
| Upper lid crease | none | none |
|
 |
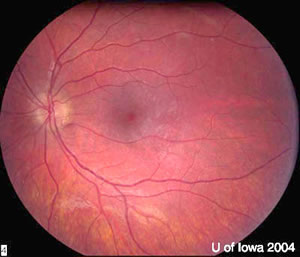 |
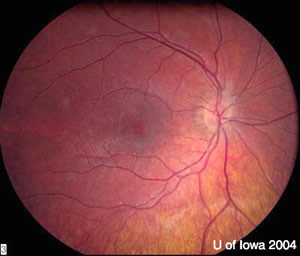
| OD | OS |
There is a faint speckled pigmentary retinopathy evident in the periphery—a light "salt and pepper change". Dr. Weingeist says this retinopathy is not as dramatic as the bone spicules seen in retinitis pigmentosa.
 |
Dr. Nerad emphasizes that there are two primary forms of ptosis: congenital ptosis and involutional ptosis. Congenital ptosis is manifested at birth and is associated with poor levator function and absent upper lid crease. Involutional ptosis is associated with good levator function and high upper lid crease and occurs in the elderly due to dysfunction or dehiscence (which is hardly never seen at the time of surgery) of the levator muscle. If the patient does not fit one of these two most common causes of ptosis, then the clinician needs to consider one of the less common causes of ptosis.
Clinicians who are "lumpers" would categorize this patient as having Chronic Progressive External Ophthalmoplegia (CPEO) with varying risk of developing other organ system involvement. Those who are "splitters" would say that he has Kearns-Sayre syndrome, a subset of CPEO that places him at high risk for sudden cardiac death. In either case, cardiac and endocrine workups are required. Because this is a mitochondrial disease, any organ system may be affected.It is important to remember that these patients can die from: 1) sudden cardiac death due to 1 st degree A-V block; and 2) hyperglycemic acidosis after corticosteroid administration. This becomes particularly important in light of the fact that myasthenia gravis is on the differential diagnosis list.
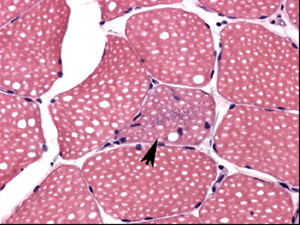
The use of Tensilon (edrophonium) is worrisome in these patients as it may precipitate heart block and arrhythmias.It is also worrisome that these patients may suffer sudden cardiac death, even if cardiac evaluation results are normal. For this reason, some electrophysiologists recommend prophylactic pacemaker placement for these patients.The diagnosis is aided by histopathology of skeletal muscle fibers (usually obtained from the thigh) that show ragged red fibers. These fibers represent abnormal mitochondrial respiratory chain function. They are found in all mitochondrial myopathies.
These disorders (e.g., CPEO, MERRF, etc...), although clinically different, are quite similar on a molecular level and considered by some to be the same disease with variable phenotypic expression based on the organ systems most heavily involved.Because the defect resides within mitochondrial DNA, affected males should not pass on this disease. Affected females may pass on this disease if the fertilized egg contains a sufficient percentage of abnormal mitochondrial DNA (heteroplasmy).
EPIDEMIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT
|
Pramanik S, Nerad JA. Chronic Progressive External Ophthalmoplegia (CPEO) - Kearns-Sayre Syndrome: 12-year-old boy with painless, progressive ptosis OU over 3 years. EyeRounds.org. March 26, 2005; Available from: http://www.EyeRounds.org/cases/case24.htm.

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links

