Contributors: Thomas J.E. Clark, MD; Erin M. Shriver, MD, FACS
The University of Iowa
Department of Ophthalmology and Visual Sciences
Step 1: ALWAYS clear the globe
Step 2: History
Patient age
Mechanism of injury
What type of object inflicted the injury?
Dog bites:
Recommend the dog be put down as the second bite is many times worse than the first
Give antibiotics covering mixed flora (e.g. Streptococcal spp., Anaerobes, Pasteurella, and gram negative rods (GNR))[1]:
Ampicillin/Sulbactam (Unasyn®): 1.5-3gm IV q6h [adults], 150-300mg/kg/d IV divided q6h [pediatrics]
Amoxicillin/Clavulanate (Augmentin®): 875mg/125mg PO bid [adults], 25mg/kg/d PO divided bid [pediatrics]
Meropenem: 500mg IV q8h [adults] with dose adjustment for CrCl <51mL/min, 10mg/kg (max dose: 500mg) IV q8h [pediatrics]
Moxifloxacin: 400mg IV or PO qd [adults], contraindicated in pediatrics
Clindamycin (misses GNR and Pasteurella): 600-900mg IV q8h or 300-450mg PO q6h [adults], 20-40mg/kg/d IV or 8-16mg/kg/d divided in 3 or 4 equal doses [pediatrics]
Is there a potential for retained foreign body (metal vs organic material)?
Time lapse since injury occurred
Last oral intake
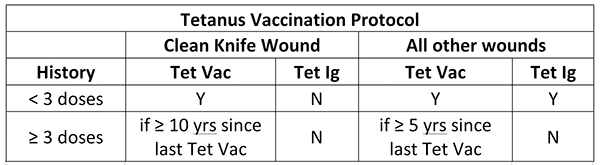
Last Tetanus shot (see Tetanus Vaccination Protocol below)
Step 3: Exam
Take a picture
Look for RED FLAGS that warrant Oculoplastic involvement
Visible orbital fat (signifies septal violation concerning for damage to deeper structures)
Laceration of the eyelid margin (requires meticulous closure to avoid long-term sequelae from lid margin notching)
Damage to the lacrimal system (shearing forces commonly damage the medial canthal structures) – may need to probe and irrigate to rule out canalicular involvement
Supplies needed for lacrimal system probing and irrigation:
4% topical lidocaine
Cotton-tipped applicator
Punctal dilator
Bowman probe (size 00 or 0)
23-gauge curved lacrimal cannula on a 3cc syringe filled with fluorescein-infused saline (this can be created with saline and a standard fluorescein strip)
Step 4: Repair
Obtain consent
Take a photo
Obtain necessary materials:
Lidocaine (1% or 2% with 1:100,000 epinephrine)
20- and 27- or 30-gauge needles [draw with 20-gauge, administer with 27- or 30-gauge]
3mL or 5mL syringe
Sterile saline with irrigation tip
5% Betadine (Povidone-iodine)
0.5% topical proparacaine drops
Castroviejo needle holder
Paufique forceps
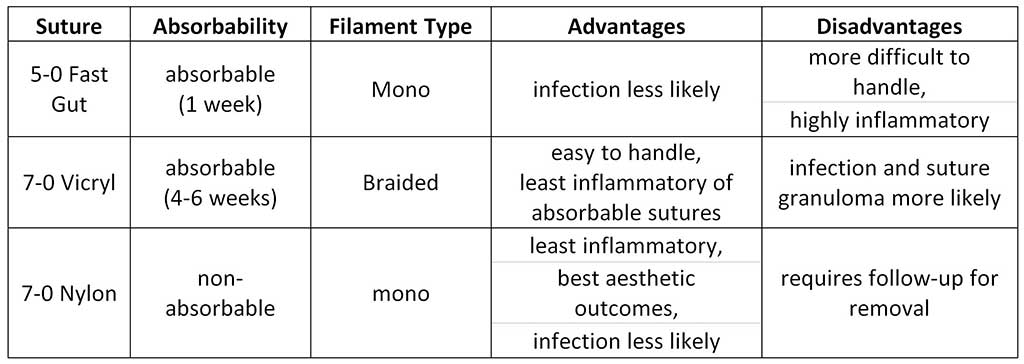
Suture (5-0 or 6-0 Fast vs 7-0 Vicryl vs 7-0 nylon
Straight scissors
Sterile gloves
Mask
Erythromycin ointment
Sterile eye drape
Sterile gauze and cotton-tipped applicators
Mayo stand and sterile drop cloths, if available (if not, can set instruments and supplies on the opened sterile gloves wrapper)
Anesthetize
Explore
Irrigate with copious amounts of sterile saline
Anti-sepsis: prep with 5% Betadine until the tissue bleeds
Prepare a sterile surgical field utilizing a Mayo stand with sterile drop cloths (can then open and arrange instruments and suture), sterile gloves, mask, and sterile drape
Close the wound
General principles [2]
Tissue is almost never missing
Strive for tension-free closure to avoid lagophthalmos/exposure keratopathy
Unless completely unavoidable, avoid making vertically-oriented suture passes as closing a horizontally-oriented wound with vertically-oriented suture passes can cause vertical cicatrization resulting in ectropion/lagophthalmos/exposure keratopathy
Cicatricial changes pull the lower lid down—attempt to elevate the lower lid as much as possible during repair (in cases of unavoidable vertical tension, a frost suture or temporary tarsorrhaphy may need to be placed)
NEVER suture the orbital septum
Suture selection considerations
Patient expectations regarding scarring
If aesthetics are important to the patient and the patient is able to return to clinic in order to have the sutures removed, non-absorbable monofilament sutures (e.g. nylon or prolene) are preferrable
Patient reliability for follow-up
Avoid non-absorbable sutures in patients unlikely to return for removal
Amount of tension
Braided sutures are superior for wound closure on tension
Complexity of laceration/necessity of both deep and cutaneous closures
Use 5-0 or 6-0 Vicryl for deep closures
Suturing technique
Simple, interrupted closure is sufficient and preferable in most cases
Divide the wound in half with the first suture pass, then continue to halve the remaining unclosed wound segments
For extensive lacerations, a running closure is more expedient
Can use a combination of interrupted and running closures, with interrupted sutures placed at points of tension and locations where the laceration changes direction
Apply erythromycin ophthalmic ointment to the wound
If the patient has an erythromycin allergy, can use bacitracin ointment or Polysporin® (bacitracin + polymyxin B) ointment
*Table adapted from Lee & Carter, 2006 [3]
Step 5: Post-closures cares/follow-up
Apply erythromycin (vs bacitracin vs Polysporin®) ophthalmic ointment to the wound TID
Arrange follow-up in Oculoplastics clinic within 10 days
Remove sutures (if Vicryl or nylon were used) 6-10 days post-operatively
Step 6: Wound management/scar maintenance
Avoid direct sunlight exposure for at least 6 months
Once wound is healed… MASSAGE, MASSAGE, MASSAGE
20 strokes TID
Topical vitamin E or Mederma®
*Tet Vac
if < 7 years old, give DTap
if > 7 years old with noprior Tdap, give Tdap
if > 7 years old with prior Tdap, give Td
^Tet Ig
give 250 Units IM at site away from Tet Vac site
if no Tet Ig available, give Tet IVIg
Table adapted from CDC, 2011 [4]
Table adapted from CDC, 2011 [4]
References
Stevens DL, Bisno AL, Chamber HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Disease Society of America. Clin Infect Dis. 2014;59:e10-52.
Nerad JA. Chapter 13. Eyelid and Orbital Trauma. IN: Techniques in Ophthalmic Plastic Surgery—A Personal Tutorial. Elsevier , 2010; pp 355-369.
Lee J, Carter KD. Chapter 6. Suture Materials and Needle. IN: Basic Principles of Ophthalmic Surgery, TA Oetting (Second Ed.) American Academy of Ophthalmology, 2006, 2011; pp 83-89.
Centers for Disease Control and Prevention (CDC). Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis (Tdap) vaccine from the Advisory Committee on Immunization Practices 2010. MMWR Morb Mortal Wkly Rep. 2011;60:13.
Suggested Citation Format
Clark TJE, Shriver EM. Emergent Evaluation of Eyelid Lacerations: A guide for ophthalmology residents. EyeRounds.org. December 17, 2015; Available from: http://www.EyeRounds.org/tutorials/eyelid-lacerations
University of Iowa
Roy J. and Lucille A. Carver College of Medicine
Department of Ophthalmology and Visual Sciences
200 Hawkins Drive
Iowa City, IA 52242
University of Iowa
Roy J. and Lucille A. Carver College of Medicine
Department of Ophthalmology and Visual Sciences
200 Hawkins Drive
Iowa City, IA 52242