Functional Visual Loss
Functional Visual Loss
John J Chen, MD, PhD and Yanjun (Judy) Chen, MD, PhD
March 6, 2013
Chief complaint: “I can’t see anything.”
History of Present Illness: A 37-year-old male presented with decreased vision for the past 10-15 years, which had been progressively worsening over the past year. The patient was referred by his local optometrist because he could not read any of the letters on the chart and showed no improvement with refraction. He was referred for visual loss with a high suspicion for functional visual loss.
Past Ocular History: None
Past Medical History: Mild mental retardation and developmental delay, schizophrenia
Medications: Olanzapine
Allergies: None
Family History: Non-contributory
Social History: Disabled, semi-independent living. He denied alcohol or tobacco use.
Review of systems: As above, otherwise negative
Ocular exam
Visual Acuity:
- Right eye (OD): Hand motion
- Left eye (OS): Hand motion
- Despite claiming hand motion vision, he was able to check boxes on a questionnaire sheet. In addition, he was able to ambulate in an unfamiliar environment without difficulty.
- On formal testing, he claimed that he was unable to see the optokinetic drum. However, he had appropriate nystagmus to the optokinetic drum.
- He saw two eye charts with a vertical prism placed over one eye.
Pupils: 5→3, no Relative Afferent Pupillary Defect (RAPD), both eyes (OU)
Extraocular movements: Full
Confrontation visual fields: Unable to count fingers, but able to track objects placed in all four quadrants.
Intra-ocular pressure:
- OD: 10 mmHg
- OS: 17 mmHg (squeezing)
External: Normal
Slit Lamp Exam: Unremarkable except mild para-central thinning of the cornea in both eyes.
Dilated Fundus Exam
Normal appearing optic nerves with cup-to-disc ratio of 0.2 in both eyes. The maculae were normal. The vessels and peripheral retina were normal.
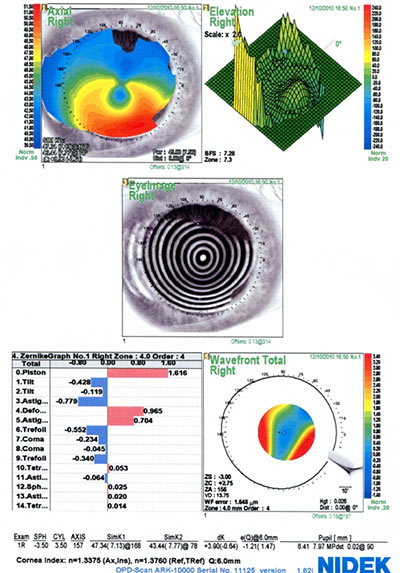
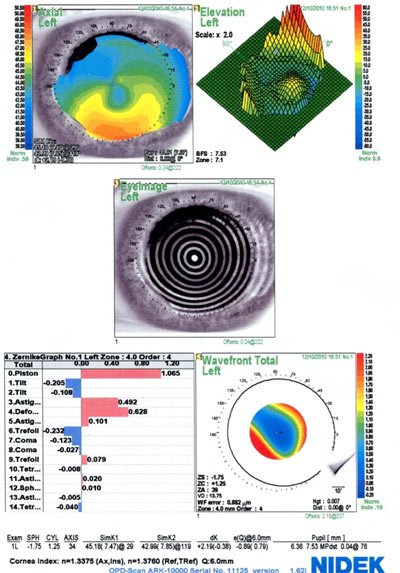
Retinoscopy was performed given that the evaluation of subjective visual function was unreliable. The retinoscopy exam revealed an irregular reflex with scissoring in both eyes. This finding raised a suspicion of corneal irregularity as the cause of the decreased vision. Corneal topography showed asymmetric inferior steepening consistent with keratoconus or pellucid marginal degeneration (Figure 1).
We were unable to perform a manifest refraction because he stated that things were blurred and refused to acknowledge counting fingers. However, when we gave him a trial frame with the estimated refraction from the corneal topography, he was very satisfied with the outcome. He said he was seeing the best that he had in years. Although his best visual outcome would likely be achieved by the use of rigid gas permeable contact lenses due to his underlying keratoconus, he would be a poor candidate for this option due to his inability to manage contact lenses. Providing astigmatic correction with glasses appeared to have improved his visual acuity and will remain a viable treatment option.
Diagnosis: Keratoconus masked by functional overlay.
Although there was clear functional overlay, the patient had true ocular pathology causing decreased vision. This case was challenging in that the reliability of the visual function testing was limited by his decreased mental capacity and poor cooperation. It would be easy to ignore his complaints of blurred vision because of the obvious discordance between his behavior and expressed visual capacities; although his visual acuity was measured hand motion, he clearly demonstrated ability to ambulate through unfamiliar territory, shake hands, and touch the examiner’s finger reliably in various positions.
Keratoconus appeared to contribute to the visual decline, based on ocular exam findings of paracentral corneal thinning and irregular retinoscopic reflex, as well as corneal topography finding of asymmetric steepening inferiorly.
Discussion
Functional visual loss refers to a decrease in visual acuity or loss of visual field with no underlying physiologic or organic basis. Patients with functional visual loss make up 1-5% of the referrals to ophthalmologists.[1,2] The highest incidence occurs in 11-20-year-old patients with a female predominance (63%).[3] The average workup for a patient with functional visual loss is greater than $500 and likely millions of dollars are spent on fraudulent disability claims.[4] A thorough clinical examination can avoid unnecessary investigations and disability expenditures, therefore saving society money as a whole.
First and foremost, the diagnosis of functional or nonorganic visual loss is one of exclusion. There is often an underlying true organic visual problem that is masked by functional complaints, and the main goal of any examination is to find the kernel of truth. Functional visual loss can be seen in a variety of patients. There can be a conscious purposeful report of decreased vision in malingering patients, such as patients seeking disability or monetary gain. A nonorganic report of decreased vision can also be part of a somatization disorder. Regardless of the etiology, it is important to have a repertoire of tests to differentiate true functional visual loss from organic visual loss. The approach and tests performed depends on the patient’s complaint and can be broken down into two broad categories: decrease in visual acuity and loss of visual field. These can be further stratified between monocular or binocular visual loss and the degree of visual impairment.
Binocular blindness
- Nonvisual tasks:
- The examination starts as the patient walks into the room, observing his ability to navigate to the chair and to shake hands. Appearance and demeanor of the patient can also contribute. For instance, it was shown that patients wearing sunglasses to a tertiary neuro-ophthalmology practice were more likely to have functional visual loss.[5]
- Fingertip touching: A patient with true binocular blindness can still touch their index fingers of opposite hands together because this task is based on proprioception and not visual cues. Patients with functional binocular blindness will often claim they are unable to do this.
- Sign signature: Same principal as fingertip touching. This can be done in a patient with true binocular blindness.
- Mirror test:
- If the vision is at least light perception, moving a mirror in different angles will result in non-suppressible nystagmoid movements as the eyes follow the moving reflections.
- Sudden unannounced placement of a mirror in front of the patient may lead to accommodation, convergence, and miosis as the patient focuses on the image of themself.
- Optokinetic nystagmus drum: Induced jerk nystagmus indicates at least 20/400 vision.
- Shock value test: These include a variety of tests including the menace reflex where the examiner presents visual threats such as a closed fist and observes for blinking or flinching. The examiner can also suddenly drop an object to see if a patient will reflexively react.
Monocular blindness or visual impairment
- Relative afferent pupillary defect (RAPD): This is the most important objective test that can be performed if the patient claims to have a large difference in visual acuity between the two eyes. If there is no refractive error or media opacity causing the disparity in acuity, a RAPD will likely be present in the affected eye if there is true pathology.
- Fogging test:
- This can be done by placing a plus lens (≥+5.00D over the normal refractive correction) in front of the good/unaffected eye and a lens with minimal power over the affected eye. The patient is then asked to read the chart with both eyes. The patient may not realize that the unaffected eye is fogged and a patient with functional monocular visual loss often reads well with the “affected” eye.
- Paired cylinders can also be used. A plus cylinder and a minus cylinder of the same power are placed in parallel in front of the good/unaffected eye. While the patient reads the chart, the axis on one cylinder is rotated 10-15 degrees to fog the good/unaffected eye. If the patient continues to read the chart successfully, they are revealing adequate vision in the “affected” eye.
- Titmus stereopsis test: Stereopsis requires binocular vision. Ability to see 9/9 circles requires 20/20 vision in both eyes. Visual acuity can be estimated based on stereopsis (see Table 1).
- Prism tests:
- Base-out prism test: A 10-prism diopter lens placed base-out in front of one eye should normally elicit a movement of both eyes toward the direction of the apex of the prism followed by a shift of the fellow eye back toward the center. A true loss of monocular vision will not result in conjugate movement when the prism is placed over the affected eye.
- Vertical prism dissociation test: A 4-prism diopter lens is placed base-down in front of the good/unaffected eye. A 20/20 or larger size Snellen is projected. If the patient is able to see two letters of equal clarity, it establishes good vision in the affected eye.[6]
- Red-Green duochrome test: The patient is given red-green glasses with the red lens over the affected eye. The patient is asked to read the red-green duochrome chart with both eyes. The eye behind the red lens is able to see letters on both sides of the chart, whereas the eye behind the green lens can only see letters on the green side of the chart. If the patient is able to read all of the letters, this demonstrates that the affected eye is able to read the letters displayed.
- Color plate test: The patient is given red-green glasses with the red lens over the affected eye. The Ishihara plates cannot be seen by the eye with the green filter. Ability to read the colors indicates at least 20/400 vision in the affected eye.
- Cycloplegic test: For younger patients with the ability to accommodate, a cycloplegic test can be used. Place tropicaimide in only the good eye and saline in the affected eye. After accommodation is paralyzed, check the patient’s visual acuity at near with both eyes open. The patient may not realize that they are only reading with the affected eye and may demonstrate good near visual acuity.
- Caveat: high myopes will still have good near vision after cycloplegia.
Table 1: Relationship of visual acuity and stereopsis
| Visual acuity |
Average Stereopsis (seconds of arc) |
Titmus stereopsis |
20/20 |
40 |
9/9 circles |
20/25 |
43 |
8/9 circles |
20/30 |
52 |
8/9 circles |
20/40 |
61 |
7/9 circles |
20/50 |
78 |
6/7 circles |
20/70 |
94 |
5/9 circles |
20/100 |
124 |
3/3 animals or 4/9 circles |
20/200 |
160 |
3/9 circles or 2/3 animals |
| -Modified from [7] |
Bilateral visual impairment
- Bottom-up visual acuity testing: Begin with the smallest line (20/10 if available). Progressively increase the size saying that the size is “doubled” in size and express astonishment that the letters cannot be seen. This can often uncover better visual acuity than top-down visual acuity testing in patients with functional vision loss.
- “Vision aids”: The patient is given trial frames with four lenses equaling the correct prescription and told that the lenses are special magnifying lenses. This may lead to improvement in visual acuity indicating a nonorganic component.
- Near vision testing: A large discrepancy between near-visual acuity and distance acuity provides evidence of nonorganic disease.
- Stereopsis: see above. As mentioned above, this also can provide an assessment of visual acuity (Table 1).
- Size consistency test: Evaluate a patient’s ability to read the Snellen chart at 20 feet and then at 10 feet. The patient should be able to read letters half the size of the letters read at the full distance. A patient with functional visual loss will often not admit to being able to read the smaller optotypes regardless of the proximity to the target.
Visual field loss
- Saccade test: Test saccadic eye movements into the reported absent portion of the field. A patient with nonorganic visual field loss may demonstrate accurate saccades to targets in the “nonseeing” field because they are assuming eye movements and not visual fields are being tested.
- Confrontation testing:
- The examiner asks the patient to count fingers in the “non-seeing” field and instructs to report “none” when none are seen. As the test progresses, the examiner changes to showing fingers silently. A patient response of “none” when the fingers are silently displayed in the “non-seeing” field confirms vision in that area.
- Monocular and binocular visual field testing: If the patient reports a monocular visual field defect, the visual field test can be repeated with both eyes open. If the field defect is still present under binocular testing, the monocular defect can be assumed nonorganic. This can be done with confrontation visual field testing or with formal evaluation such as Humphrey or Goldmann visual field testing.
- Goldmann visual field testing: Nonorganic visual fields often demonstrate a spiraling field that becomes smaller as the test object is moved around the field. Crossing isopters or a visual field that remains the same size regardless of the size or brightness of the test stimulus (yielding isopters nearly one on top of another) is also often seen in functional visual field loss.
- Tangent screen: A tangent screen test can be performed at two different distances from the screen (usually 1 and 2 meters) while maintaining the same ratio of target size to target distance (i.e., larger target at further distance). A patient with organically constricted visual fields will show an increase in the size of the visual field when moved to a farther distance while a patient with functional visual field loss will often report the same absolute size of the field (tubular or gun-barrel field).
- A nonorganic tubular visual field can also be elicited with repeated confrontation visual field testing at 1 meter and at 2 meters from the patient.
Other tests
In addition to the above examination techniques, retinal imaging and electrophysiological testing can be helpful in elucidating functional vision loss from true organic vision loss. Optical coherence tomography can help identify optic nerve and retinal pathology.[8] In addition, fundus autofluorescence is very sensitive in detecting subtle macular pathology.[9] Multifocal electroretinogram is able to detect focal problems of the rods and/or cones within the macula, although responses can be voluntarily suppressed.[10,11] Visually evoked potentials, which measure the speed of signal from the optic nerve to the occipital cortex, can also be helpful in some circumstances in differentiating nonorganic vision loss from true pathology.[12-15]
Management
Reassurance alone is the best treatment. Providing nonspecific treatments, like glasses or eyedrops, provides a mixed message to the patient and is less effective than reassurance alone.[16,17] It is important to stress a good prognosis, which provides “a way out” and gives the patient the opportunity to recover.[18] Confrontation is rarely helpful.[19] Between 45% and 78% of patients will experience resolution of their visual symptoms with reassurance alone.[3,18,20,21] However, some patients will continue to have persistent functional visual loss, especially in patients with co-existing psychiatric disease or in patients with motivation for material secondary gain. Adults are more likely to have underlying psychiatric illness compared to children. Concomitant psychosocial stressors are more likely in children, while adults often develop functional visual loss after trauma.[3]
Once functional visual loss is diagnosed, it is important to schedule at least one follow-up appointment to maintain a rapport with the patient and also to ensure that there is no organic disease underlying the symptoms. It is estimated that approximately 2% of patients with a diagnosis of functional visual loss have true organic disease.[3] Common masqueraders include keratoconus, cone dystrophy, Stargardt disease, amblyopia, paraneoplastic syndromes, small occipital infarcts, and acute zonal occult outer retinopathy.
Diagnosing functional visual loss is an important skill that can begin the healing process for the functional patient. Using the appropriate clinical tests can obviate the need to perform expensive investigations, such as magnetic resonance imaging, and avoid false disability expenditures, therefore saving society money as a whole.
Differential Diagnosis
True organic disease, commonly keratoconus, cone dystrophy, Stargardt disease, amblyopia, paraneoplastic syndromes, small occipital infarcts, and acute zonal occult outer retinopathy.
Epidemiology
- 1-5% of referrals to ophthalmologists.
- Highest proportion in 11-20-year-old patients, but can occur at any age.
- 63% female
|
Symptoms
- Binocular or monocular decreased vision and/or visual field loss
|
Signs
- See above for clinical tests
|
Treatment
- Reassurance with appropriate follow-up
|
References
- Bose S, Kupersmith MJ. Neuro-ophthalmologic presentations of functional visual disorders. Neurol Clin 1995;13(2):321-3
- Schlaegel TF, Jr., Quilala FV. Hysterical amblyopia; statistical analysis of forty-two cases found in a survey of eight hundred unselected eye patients at a state medical center. AMA Arch Ophthalmol 1955;54(6):875-84.
- Lim SA, Siatkowski RM, Farris BK. Functional visual loss in adults and children patient characteristics, management, and outcomes. Ophthalmology 2005;112(10):1821-8.
- Keltner JL, May WN, Johnson CA, Post RB. The California syndrome. Functional visual complaints with potential economic impact. Ophthalmology 1985;92(3):427-35.
- Bengtzen R, Woodward M, Lynn MJ, Newman NJ, Biousse V. The "sunglasses sign" predicts nonorganic visual loss in neuro-ophthalmologic practice. Neurology 2008;70(3):218-21.
- Golnik KC, Lee AG, Eggenberger ER. The monocular vertical prism dissociation test. Am J Ophthalmol 2004;137(1):135-7.
- Levy NS, Glick EB. Stereoscopic perception and Snellen visual acuity. Am J Ophthalmol 1974;78(4):722-4.
- Sakata LM, Deleon-Ortega J, Sakata V, Girkin CA. Optical coherence tomography of the retina and optic nerve - a review. Clin Experiment Ophthalmol 2009;37(1):90-9.
- Schmitz-Valckenberg S, Holz FG, Bird AC, Spaide RF. Fundus autofluorescence imaging: review and perspectives. Retina 2008;28(3):385-409.
- Lai TY, Chan WM, Lai RY, Ngai JW, Li H, Lam DS. The clinical applications of multifocal electroretinography: a systematic review. Surv Ophthalmol 2007;52(1):61-96.
- Vrabec TR, Affel EL, Gaughan JP, Foroozan R, Tennant MT, Klancnik JM, Jr., et al. Voluntary suppression of the multifocal electroretinogram. Ophthalmology 2004;111(1):169-76.
- Bobak P, Khanna P, Goodwin J, Brigell M. Pattern visual evoked potentials in cases of ambiguous acuity loss. Doc Ophthalmol 1993;85(2):185-92.
- Gundogan FC, Sobaci G, Bayer A. Pattern visual evoked potentials in the assessment of visual acuity in malingering. Ophthalmology 2007;114(12):2332-7.
- Leavitt JA. Diagnosis and management of functional visual deficits. Curr Treat Options Neurol 2006;8(1):45-51.
- Rover J, Bach M. Pattern electroretinogram plus visual evoked potential: a decisive test in patients suspected of malingering. Doc Ophthalmol 1987;66(3):245-51.
- Kathol RG, Cox TA, Corbett JJ, Thompson HS. Functional visual loss. Follow-up of 42 cases. Arch Ophthalmol 1983;101(5):729-35.
- Thompson HS. Functional visual loss. Am J Ophthalmol 1985;100(1):209-13.
- Chen CS, Lee AW, Karagiannis A, Crompton JL, Selva D. Practical clinical approaches to functional visual loss. J Clin Neurosci 2007;14(1):1-7.
- Gross MP, Sloan SH. Patients with eye symptoms and no organic illness: an interdisciplinary study. Psychiatry Med 1971;2(4):298-307.
- Kathol RG, Cox TA, Corbett JJ, Thompson HS, Clancy J. Functional visual loss: II. Psychiatric aspects in 42 patients followed for 4 years. Psychol Med 1983;13(2):315-24.
- Sletteberg O, Bertelsen T, Hovding G. The prognosis of patients with hysterical visual impairment. Acta Ophthalmol (Copenh) 1989;67(2):159-63.
Suggested citation format:
Chen JJ, Chen Y. Functional Visual Loss. EyeRounds.org. March 6, 2013; available from: http://www.EyeRounds.org/cases/165-functional-visual-loss.htm
last updated: 03/06/2013
Image Permissions:

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.