
Chief Complaint: Poor vision and severe ocular itching.
History of Present Illness: A 52-year-old Caucasian male presents to the cornea clinic with a chief complaint of vision loss. In addition to his vision loss, he complains of itchy eyes and mucoid discharge. He also reports a history of waxing and waning eczema over the past decade. Two years prior to this visit, he presented with similar symptoms and was treated with medroxyprogesterone and fluoromethalone (FML) three times a day in both eyes. This medical regimen improved his symptoms. Unfortunately, the patient discontinued his ocular prescription and was lost to follow-up after the initial visit.
Past Ocular History: Unremarkable for surgery or trauma.
Medical History: History of uncontrolled eczema for the past decade.
Medications: He uses artificial tears as needed. Otherwise, he takes no medications or other eye drops.
Family History: Father with cataract. No other pertinent family history.
Social History: The patient is a habitual smoker (1 pack per day).
 |
 |
 |
 |
 |
 |
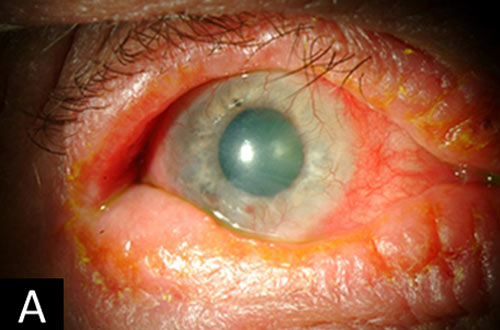
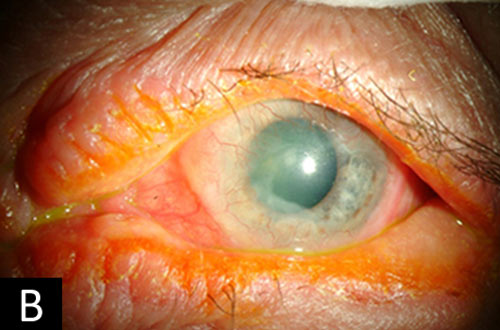
The symptoms of itching and findings of chronic conjunctivitis, eczema, symblepharon, pannus, and posterior subcapsular cataract are consistent with a diagnosis of atopic keratoconjunctivitis. At the patient’s initial visit two years prior, his condition was moderately severe (figures 1A and B). He was treated with low potency topical corticosteroids (FML and medroxyprogesterone) which resulted in improvement in his symptoms. However, he discontinued these medications sometime after he was lost to follow up. Unfortunately, his disease progressed at a rapid rate over the next two years. His symptoms became severe enough that he decided to return for an examination. On exam at this time, the conjunctiva had entered the visual axis, and his visual acuity had significantly decreased (figures 1C and D).
Atopic keratoconjunctivitis (AKC) is a chronic inflammatory disease of the eye that occurs predominately between the late teenage years and the fifth decade of life.[1] It is a chronic, bilateral disease that relapses and remits with little to no seasonal correlation (as opposed to vernal keratoconjunctivitis). Atopic dermatitis is present in 95% of cases and asthma in 87% of cases.[2] Incidence of AKC increases with a family history of atopic disease.[1] The primary symptom is ocular itching. Mucoid discharge and tearing are other common symptoms. Periocular eczema is almost always present. Lid manifestations include hypertrophy, crusting, cicatrization, ectropion, and madarosis. Conjunctivitis of the palpebral, bulbar, and limbal conjunctiva is present in varying degrees. Palpebral conjunctivitis is characterized by micropapillae of the tarsal conjunctiva – primarily of the lower eyelid. Bulbar conjunctivitis includes hypertrophy of conjunctiva with excess mucous. Symblepharon, adhesion of the palpebral conjunctiva to the bulbar conjunctiva, occurs in approximately 20% of cases.[3] Corneal neovascularization related to stem cell deficiency occurs in approximately 60% of cases.[3] Corneal ulcers and erosions are more common due to the poor epithelial adhesion and predispose to infectious keratitis, which can permanently scar the corneal stroma and/or lead to corneal perforation. Posterior subcapsular cataracts are also common in these patients.
The pathogenesis of atopic keratoconjunctivitis has not been fully elucidated. In simple terms, the disease originates from a disorder of the adaptive immune system in predisposed individuals. An admixture of mast cells, Th1 T-cells, Th2 T-cells, and eosinophils is present on biopsy of the conjunctival epithelium.[1] This helps aid in the diagnosis. However, the diagnosis of AKC is made clinically, based on both a history of atopy and the ocular examination.
Management of atopic keratoconjunctivitis is aimed at decreasing the inflammatory response and controlling symptoms. The majority of cases are co-managed with an allergist or dermatologist to provide guidance and follow up of systemic therapy. In early disease, conservative management with combination topical mast cell stabilizers and anti-histamine drops, lubricants, cold compresses, and oral anti-histamines may keep the ocular disease under control. However, in more advanced cases, additional pharmacologic therapy is necessary. Pharmacologic therapy for these cases includes topical corticosteroid drops, cyclosporine drops, or tacrolimus ointment to the eyelid skin.[2,4] When topical treatments fail to induce remission, oral prednisone, tacrolimus, or cyclosporine are the next treatment options. These are also useful for dermatologic manifestations of the disease.[5] It is important to note that as T-cells play a central role in the pathogenesis of this disease, calcineurin inhibitors such as tacrolimus and cyclosporine are an effective route for steroid-sparing therapy in both topical and systemic applications. In the final stages of atopic keratoconjunctivitis where visual loss has occurred due to corneal opacification from stem cell deficiency, the Boston keratoprosthesis may be used for visual rehabilitation in motivated patients.
Epidemiology
|
Signs
Periocular
Lids
Conjunctiva
Cornea
Lens
|
Symptoms
|
TreatmentTherapy is aimed at treating both the ocular and the systemic disease. Early disease treatment
Advanced disease treatment
|
Strobehn A, Ward M, Kitzmann A. Atopic Keratoconjunctivitis. EyeRounds.org. March 8, 2013; available from: http://www.EyeRounds.org/cases/167-atopic-keratoconjunctivitis.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
