
Multiple eyelid lesions
A 27-year-old male with a history of multiple endocrine neoplasia type 2B (MEN2B) was referred to the University of Iowa oculoplastic surgery clinic by his oncologist for a large lesion on the outer corner of his right eye. He reported that the lesion had been present for 6 months and stable in size for the 2 months prior to presentation. The patient's eyes were comfortable and he denied any tenderness, swelling, discharge, itchiness, dryness, or watering. He was seen by an outside ophthalmologist who was unable to provide a diagnosis, but offered to "cut if off".
None

Figure 1 – Full appearing lips with thickened mucosa

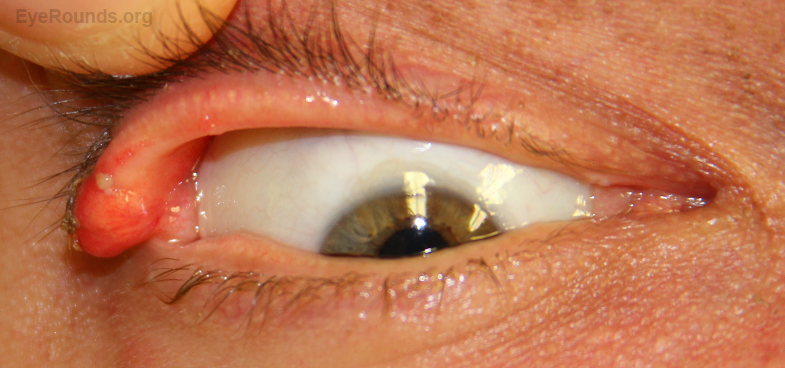
Figure 2 – A) Large, erythematous upper eyelid lesion on the lateral canthus of the right eye with a smaller upper eyelid margin lesion medial to the larger lesion. Fullness of both upper eyelids with a yellow lower eyelid lesion near the puncta with scalloping of the medial lower eyelid on the left. B) Magnified view of right upper eyelid lesion
The patient underwent incisional biopsies of the right upper and left lower eyelid lesions. ( excisional biopsy video ) The conjunctiva demonstrated papillary hyperplasia with a dense infiltrate of neutrophils on the surface and scattered neutrophils throughout the conjunctival epithelium. The underlying stroma demonstrated a circumscribed area consisting of bundles of spindle cells with fibrillary extracellular matrix and wavy slender nuclei. Cells stained positive on immunohistochemistry for S100. The diagnosis was neuroma with acute inflammation of the surrounding tissue. After a 6-month follow-up and no recurrence, he was discharged from the oculoplastics clinic. He continues close, regular follow-up with both his endocrinologist and hematologist/oncologist.
Conjunctival neuromas in the context of known MEN2B.
Multiple endocrine neoplasia (MEN) is an autosomal dominant syndrome that results in the predisposition to tumor formation in two or more endocrine glands. MEN is further classified into MEN1 (OMIM 131100), MEN2A (171400), or MEN2B (162300) based on the mutation and the type of endocrine gland tumors that the patient develops [1].
Tumors |
Mutation |
|
|---|---|---|
MEN1 |
Parathyroid glands, endocrine pancreas and duodenum, anterior pituitary, adrenal, thyroid; carcinoid tumors; lipomas and facial angiofibromas |
MEN1 gene on 11q13 |
MEN2A |
Medullary thyroid cancers, pheochromocytomas, Hirschsprung disease |
RET gene on 10q11 |
MEN2B |
Medullary thyroid cancers, pheochromocytomas, Marfan-like habitus, mucosal neuromas, intestinal ganglioneuroma, delayed puberty |
RET gene on 10q11 |
MEN2B remains a relatively rare condition with a prevalence of ∼0.2 × 10−5 and an estimated annual incidence of 4 per 100 million per year [2].
MEN2B is secondary to a germline mutation in the RET proto-oncogene on chromosome 10q11. The most common mutation (95%) is M918T in exon 16 and second most common mutation (2-3%) is A883F in exon 15 [3]. The RET gene codes for the protein RET, which is a tyrosine kinase receptor that is important for activating signaling pathways. A gain of function mutation in the RET protein leads to constitutive action of the receptor and subsequent unregulated growth resulting in the predisposition to tumor formation [4].
Mutations in the RET gene are also associated with MEN2A, Hirschsprung disease (HSCR; 142623), and medullary thyroid carcinoma (MTC; 155240) [4].
Typically, the first clinical signs of MEN2B are gastrointestinal symptoms (most commonly constipation), mucosal neuromas, and marfanoid habitus [5]. It is important to identify these patients as early as possible because they have a high likelihood (80-100%) of the development of early, aggressive medullary thyroid carcinoma (MTC). Additional signs of MEN2B include pheochromocytomas, often bilateral, and thickened corneal nerves. Characteristic physical features include full lips (see figure 1), thickened eyelids, and high-arched palate[3]. The thickening of the lips and eyelids are secondary to the mucosal neuromas.
Ocular findings include thickened corneal nerves, small plexiform and nodular subconjunctival tumors (neuromas), keratitis sicca, and thickened upper and lower lids (also related to neuromas) [6-10]. As noted above, early diagnosis is critical for these patients. Thickened corneal nerves are seen in a number of conditions including keratoconus, Noonan syndrome, multiple myeloma, leprosy, and lipoid proteinosis [11-15]. (see related atlas entry)
Any patient with clinical signs and symptoms of MEN2B should undergo molecular genetic testing of the RET gene. Additionally, any individual diagnosed with MTC should be offered testing. Genetic testing should first screen exons 16 and 15 for M918T and A883F mutations. If negative, the point mutation V804M in exon 14 should be screened followed by sequencing of the entire RET gene [4].
Before prophylactic thyroidectomy is performed, baseline calcitonin (CT) and carcinoembryonic antigen (CEA) should be measured. These are biochemical markers of MTC and are useful for follow-up after surgery [5].
If signs of pheochromocytoma are present, urinary catecholamines and catecholamine metabolites (epinephrine, norepinephrine, metanephrine, and vanillylmandelic acid) should be measured in addition to an abdominal MRI or CT [4].
From an ophthalmic perspective, if there is any doubt about the clinical diagnosis of a neuroma, excisional biopsy should be performed. Although bilaterally is more likely indicative of a systemic disease, other etiologies such as basal cell carcinoma should be ruled out. Additionally, excision may be indicated if the patient is experiencing symptomatic irritation from a lesion.
In the case that a neuroma is diagnosed on biopsy and the patient does not have a known MEN2B diagnosis, they will need a referral for systemic work-up. Ultimately the patient will need prophylactic thyroidectomy [3] as medullary thyroid carcinoma is the major cause of mortality [4]. Patients should then have annual CT scans and carcinoembryonic antigen (CEA) levels to screen for MTC relapse [5]. They need regular follow-up with a primary care provider, endocrinologist, and hematologist/oncologist. Prognosis for the patient is good with early diagnosis and surgical intervention [4].
Epidemiology
|
Signs
|
Genetics
|
Management
|
McConnell L, Hammer S, Allen RC. Multiple endocrine neoplasia type 2B: A 27-year-old male presents with multiple eyelid lesions. Posted January 23, 2016; Available from https://eyerounds.org/cases/230-MEN2B.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
