
Chief Complaint: pain, redness, photophobia of left eye
A 45 year-old male was referred to the UIHC ophthalmology department with concern for possible corneal ulcer of the left eye. His symptoms began three weeks prior with irritation, tearing, and redness. He presented to urgent care shortly after developing symptoms and was diagnosed with conjunctivitis of the left eye; he was treated with polymyxin B/trimethoprim (Polytrim) drops (1 drop in left eye every 4 hours for 5 days). He used the drops as directed and his symptoms resolved. A week later, he had recurrence of symptoms with redness of the left eye followed by irritation, pain, photophobia, and blurry vision. He also developed clear discharge with mattering in the morning. He tried using the leftover Polytrim drops and artificial tears, but with no benefit. He presented to urgent care and was referred to the UIHC ophthalmology clinic for further evaluation. He denied any problems with the right eye, previous episodes of recurrent conjunctivitis, or any symptoms of chronic dry eye in either eye. Other review of systems was only pertinent for recent nasal congestion.
Snellen
Tonopen
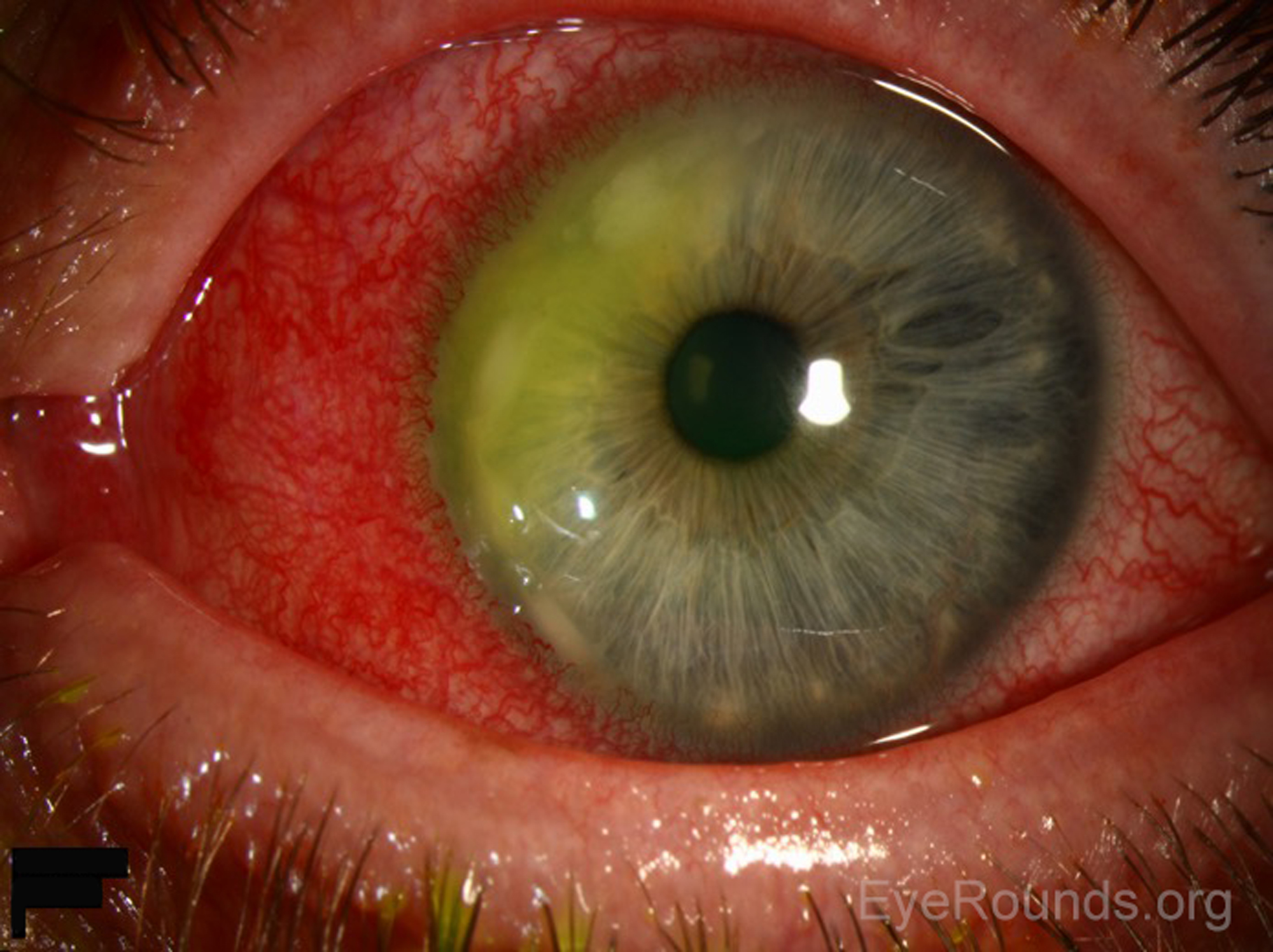
(Figure 1)
 |
 |
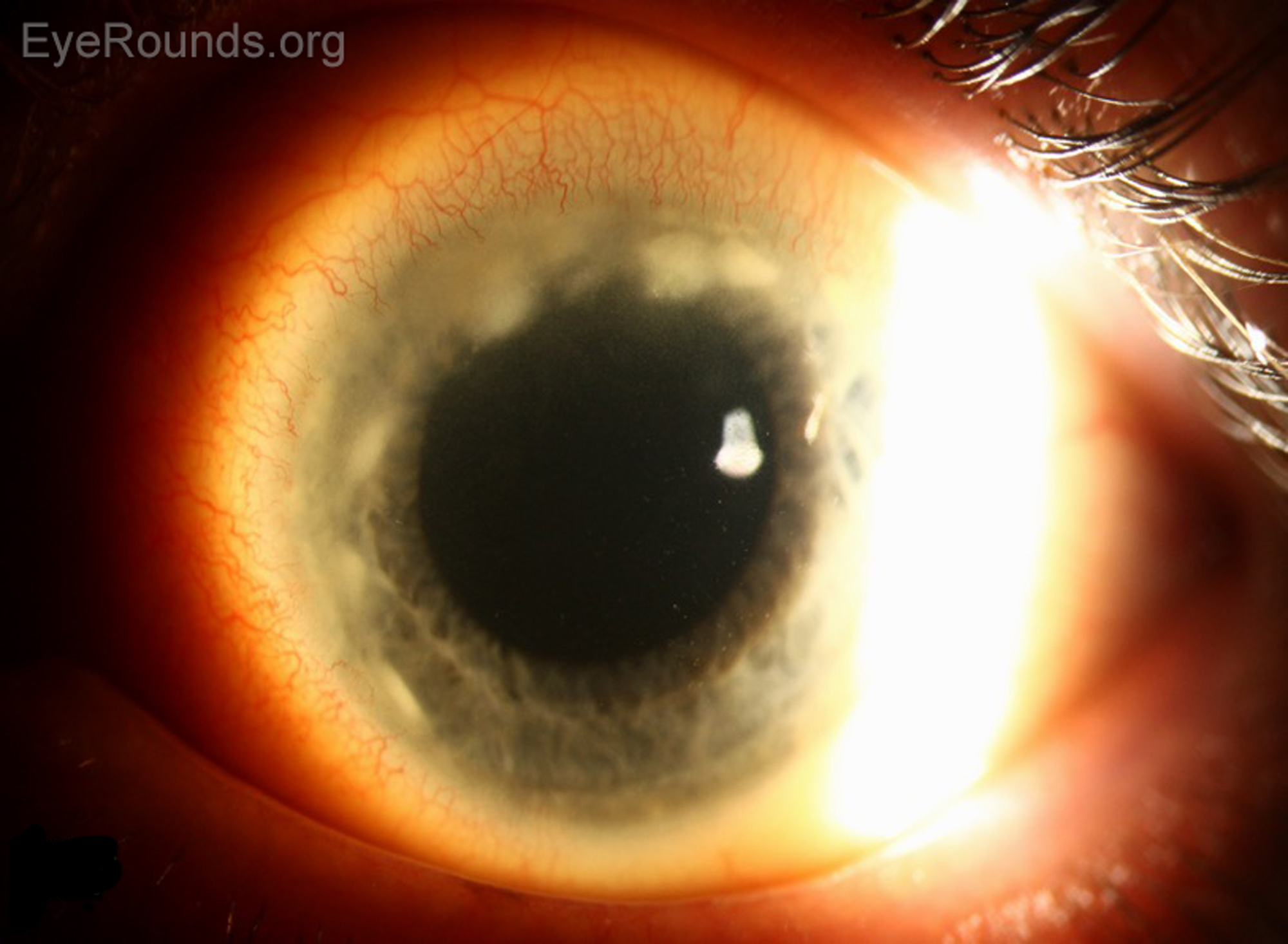
In summary, this patient was a 45 year-old male with a sub-acute presentation of redness, irritation, pain, and discharge of the left eye. On exam, he had a circumlimbal corneal infiltrate with overlying epithelial breakdown and associated conjunctival injection. He was initially started on levofloxacin every 2 hours while awake, erythromycin ointment before bed, and atropine two times daily for presumed marginal keratitis and ulceration. He returned the next day to be evaluated by the cornea service. On that exam, the circumlimbal infiltrate was still present with overlying irregular, but now closed epithelium. He developed progression of the infiltrate superiorly with two adjacent small ovoid epithelial defects at 12:30. The diagnosis of staphylococcal marginal keratitis and ulceration of the left eye was confirmed. He was continued on Levofloxacin every 3 hours while awake, Erythromycin ointment before bed, and Atropine two times a day. He was also started on prednisolone acetate 4 times a day and Doxycycline HCl 100mg by mouth two times a day. He returned two days later for follow-up with improved symptoms. On exam, the epithelial defects were fully closed and he had no corneal thinning (Figure 2). Levofloxacin and erythromycin were discontinued, atropine was continued as needed for light sensitivity, and prednisolone and doxycycline were continued. It was recommended that he start OcuSoft lid scrubs two times a day for treatment of associated blepharitis with continued close follow-up.
 |
 |
Marginal infiltrates and ulcerations are a common complication of longstanding staphylococcal blepharitis; they are also commonly referred to as catarrhal infiltrates and ulcers [1}. Catarrhal is simply referring to mucous membranes in nature, and its use in this instance is related to the etiology of the ulcer, i.e. the inflammatory response and lack of direct bacterial infection. In one study of 200 cases of ulcers at the margin of the cornea, 180 cases represented simple catarrhal ulcers and infiltrates[1]. One hundred and fifty-six of these cases were associated with chronic catarrhal conjunctivitis and 133 were associated with coagulase positive staphylococci isolated from the conjunctiva or lid margins. Additionally, concurrent blepharitis was an almost constant feature with these infiltrates and ulcerations [2]. There are case reports of patients presenting with both folliculitis and marginal keratitis, indicating that these may be associated systemic conditions. The authors of one case report speculate that there could be a common underlying process, namely an abnormal inflammatory response to bacterial stimuli, with staphylococcal aureus being the prime example of antigenic presentation [3]. This is a sensible and interesting association to consider, given that the patient in this case presentation has a past medical history of folliculitis and hidradenitis suppurativa.
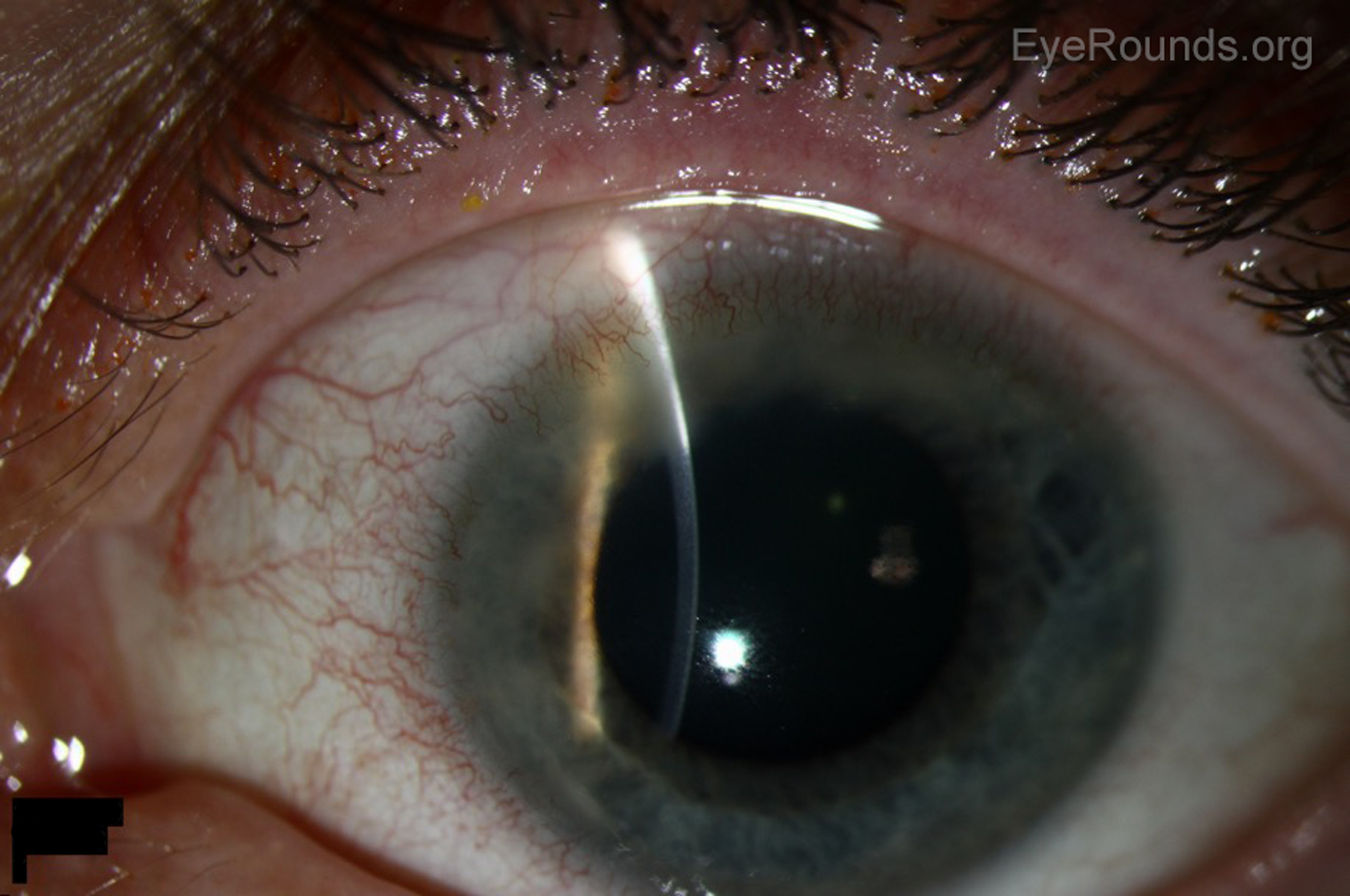
Patients often present with symptoms of pain, photophobia, and foreign body sensation [4]. The slit lamp exam most commonly shows peripheral curvilinear infiltrates in the superficial cornea (subepithelial/anterior stroma) at 10, 2, 4, or 8'oclock, where the eyelids cross the corneal periphery (figure 3). Ulcerations are located in the marginal zone and separated from the limbus by a clear corneal zone. Flourescein staining often shows epithelial defects that are smaller than the infiltrate area [5]. One study looked at 84 patients with marginal ulcers and described the appearance as single or multiple infiltrates, which subsequently coalesced with overlying epithelial breakdown of the corneal epithelium. Again, in all cases, the ulceration was separated from the limbus by clear cornea [4]. These ulcers are also characterized by circumferential progression of associated marginal infiltrates, which was seen in our patient [6]. In one study, the cases of marginal ulcers associated with chronic staphylococcal conjunctivitis also had a highly characteristic epithelial keratitis with puncate erosions on the lower half of cornea [2]. Associated findings include dilated limbal vessels, conjunctival reaction, and occasionally lid erythema and edema with reactive ptosis [4, 7-10]. Often, there are signs of staphylococcal blepharitis, meibomitis, and acne rosacea. These signs include hard scales on the lashes, collarettes, dilated vessels on lid margins, poliosis, or madarosis [2, 6, 7, 11].
 |
 |
Staph aureus is thought to be the primary inciting agent and is commonly present in the lid margins of eyes affected by marginal ulcers. In one study of marginal corneal ulcers, S. aureus was isolated from 29% of either lids or conjunctiva of those patients with corneal ulcers compared to 11% of controls [4]. In this same study, actual ulcer scrapings showed only degenerate epithelial cells, absence of cellular infiltration, and no organisms, suggesting a sterile ulcer [4]. In another study of 180 marginal ulcers, 133 had either conjunctival, lid, or ulcer scrapings with evidence of coagulase positive S. aureus [2, 8]. It has been theorized that marginal keratitis and ulceration are the result of enhanced cell mediated immunity (delayed type hypersensitivity) at the limbus to cell wall antigens and exotoxins of S. Aureus from the eyelids [5, 6, 10, 12]. The peripheral cornea is susceptible to immunologic reactions because of its proximity to limbal vasculature and conjunctival lymphoid tissue[10]. Antigen-antibody complexes are thought to be deposited in the peripheral cornea; antigen provided from the eyelids and tear film and antibody provided from limbal blood vessels [5]. One study immunized rabbits against S. aureus and then applied viable S. aureus topically to the rabbits' eyes. Of 26 rabbit eyes, 8 developed elevated nodular lesions of the cornea and 8 developed peripheral corneal infiltrates running parallel to the limbus and separated from it by a lucid interval [13]. After cessation of topical S. aureus, corneal infiltrates gradually resolved during the next 2-3 weeks. Gram stains were taken of corneal lesions in this study and showed no gram positive cocci, supporting the pathophysiology of a sterile inflammatory response rather than direct infection by S. Aureus [13]. The group of immunized rabbits was compared to rabbits who were not immunized but still had S. Aureus topically applied to the eye. The unimmunized rabbits developed conjunctival hyperemia but did not develop corneal infiltrates, suggesting that an enhanced cell mediated immune response was responsible for development of infiltrates[13]. There are also human studies that examined the theory of hypersensitivity as well. In one such study, skin testing for delayed hypersensitivity to S. aureus was performed on all subjects. The authors explained that the cell wall of S. aureus contains protein A, which specifically binds to the Fc receptor of an antibody molecule and forms immune complexes. These immune complexes act as antigen to produce a delayed hypersensitivity response [14]. The study found that 8/11 subjects with blepharitis and history of marginal keratitis were in the group that demonstrated enhanced delayed hypersensitivity reaction to the protein injected in the skin test, further supporting the theory that delayed hypersensitivity contributes to the pathogenesis of this disease [14].
The treatment of this condition focuses on addressing the two main components of the disease; the sterile corneal inflammatory reaction and the bacterial overgrowth on the eyelids. With regards to the corneal inflammatory disease, topical corticosteroids are recommended as the first-line treatment of choice. A weak topical steroid should be instilled at least 4 times a day for 1-2 weeks [5]. Low dose prednisolone (0.12%) or a stronger concentration (1%) can be used, with the former being primarily anti-inflammatory and the latter with possible immunosuppressive effects as well [7]. Some sources recommend the addition of a topical antibiotic for prophylactic and/or therapeutic benefit, especially in cases where there is epithelial breakdown [6]. If there is any question about the etiology of the infiltrate/ulcer, treatment should be initiated with antibiotic alone or in combination with steroid [10]. A study comparing prednisolone drops, neomycin, and no treatment showed that the prednisolone treatment was significantly more effective than no treatment, but there was no significant difference between no treatment and neomycin [4]. This further supports the theory that the lesions are a sterile inflammatory response that responds well to local anti-inflammatory therapy.
It is also important to reduce the antigenic burden by treating the bacterial lid disease. This treatment involves the usual blepharitis regimen, which commonly includes warm compresses and improved lid hygiene with frequent eyelid scrubs [7, 10]. Topical and/or systemic antibiotics are often added in acute presentation, with the oral antibiotic usually being a macrolide or a tetracycline [6, 7, 10]. Tetracyclines have been shown to decrease the lipolytic activity of staphylococcus organisms, which is presumed to be one of the ways the bacteria alters meibomian gland secretions and causes chronic inflammation [15]. Long-term blepharitis treatment has been shown to be effective in reducing the recurrence of marginal keratitis and ulceration [10]. One study showed pure staphylococcal marginal ulcers usually responded promptly to treatment of the associated conjunctivitis and blepharitis [2]. Regardless of the specific regimen a patient is placed on, prompt therapy addressing both the keratitis and blepharitis components will lead to a swift recovery, and steroids should be used once infectious sources have been ruled out.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Types of Peripheral Sterile Corneal Ulcers |
Description |
Staphylococcal Marginal Keratitis/Ulcer |
Peripheral curvilinear infiltrates in superficial cornea often where the lids cross the corneal periphery associated with loss of corneal epithelium; ulcerations in the marginal zone separated from the limbus by a clear corneal zone. Often associated with blepharitis. |
Mooren Ulcer |
Autoimmune. Present with severe pain, photophobia and blurred vision, circumferential peripheral stromal ulceration with undermined and infiltrated leading edge with progressive circumferential and central stromal thinning. No separation between ulceration and limbus. |
Crescentic ulceration with epithelial defect, thinning, and stromal infiltration at the limbus unexplained by ocular disease. May have extension into sclera and no separation between ulcer and limbus. Associated with systemic diseases such as RA, Wegener's granulomatosis, polyarteritis nodosa, SLE. |
|
Idiopathic thinning of peripheral cornea, often bilateral, usually painless and without inflammation, can present with visual decline/astigmatism. Fine yellow-white stromal opacities separated from limbus by a clear zone, no epithelial defect, may look like arcus senilis. |
Other disease processes in the differential diagnosis
Stiff AH, Ricca AM, Goins KM. Corneal Marginal Ulcer: Marginal keratitis with ulceration in a 45 year-old male. EyeRounds.org. posted March 14, 2017; Available from: https://eyerounds.org/cases/249-corneal-marginal-ulcer.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
