
Right eye redness and tearing
A 67-year-old woman presented for evaluation of right-sided tearing and inferior displacement of the lower eyelid. Associated with this was increased redness and itching of the right upper and lower eyelids. She reported that she constantly needed to rub her eye to alleviate the itchy feeling and wipe away tears. The patient denied pain, had no recent trauma to her periocular skin, denied any nasal congestion or rhinorrhea, and was without fevers, chills, or night sweats. She endorsed regular use of timolol-dorzolamide (Cosopt) eye drops (1 drop to the right eye, twice daily) for glaucoma and denied any new skin moisturizers, sunscreen, or makeup. The patient had been diagnosed with right lower eyelid preseptal cellulitis several months prior to presentation in the setting of a hordeolum that had subsequently resolved but she continued to have right lower eyelid ectropion. The patient was still using maxitrol (neomycin/polymyxin B/dexamethasone) ophthalmic ointment in the right eye (OD).
Right index finger: erythematous rash involving the skin of the right proximal index finger with small papules on an erythematous base, corresponding to the finger that the patient uses to rub the eye
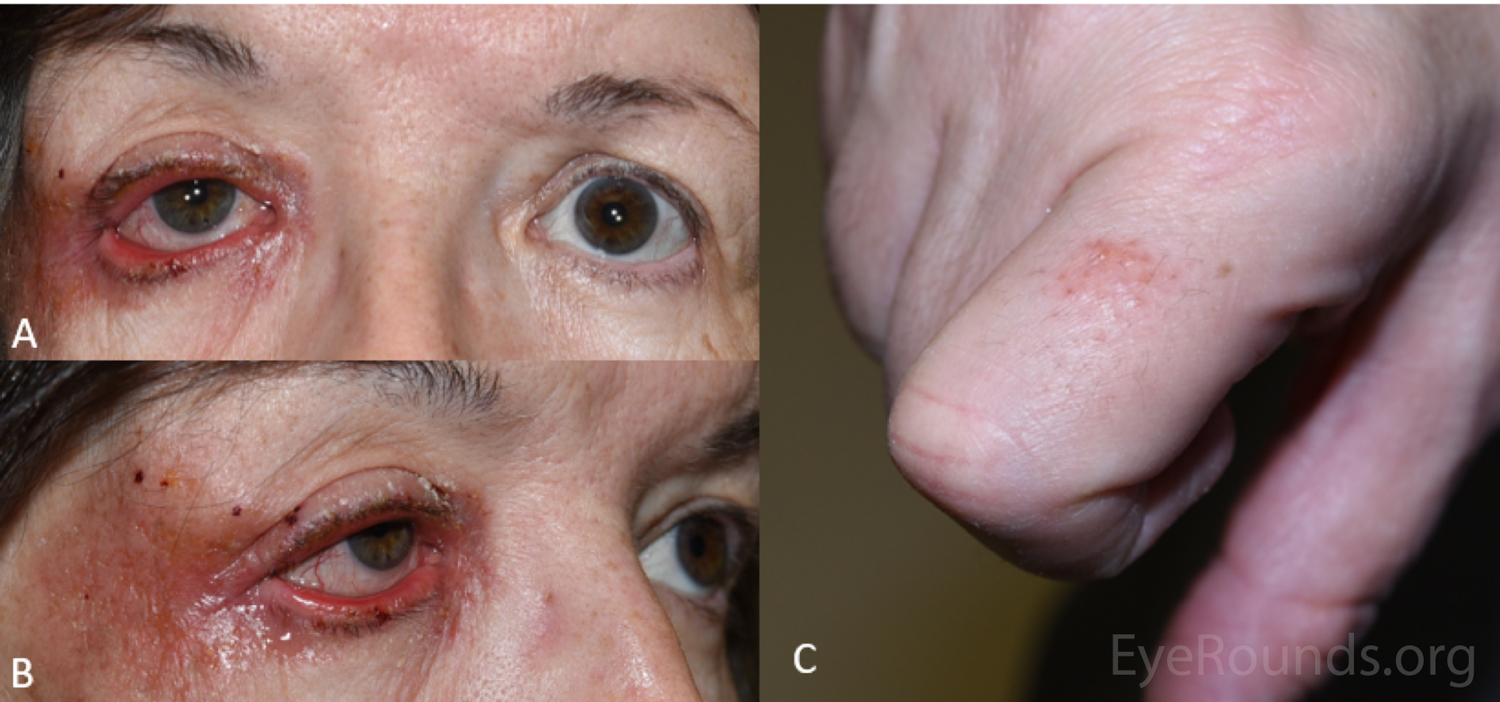
Figure 1: External photograph demonstrating rash of the right eyelid and periocular region (A and B) as well as the right proximal index finger (C).
The patient was diagnosed with periocular dermatitis presumably secondary to Cosopt (dorzolamide-timolol) drops, resulting in right lower eyelid cicatricial retraction and ectropion causing epiphora. It was recommended that the patient use petroleum jelly to provide a physical protective barrier to the skin before using Cosopt (dorzolamide-timolol) drops and she was directed to wash her face if the drops made direct contact with her skin. At nighttime she used a moisture chamber consisting of Saran wrap with tape over the affected area with lubricating drops. This improved but did not resolve her symptoms.
The patient was also referred to dermatology for additional evaluation. She underwent allergy testing, which returned positive for an allergy to phenyl mercuric acetate, which is a compound in Cosopt (dorzolamide-timolol) drops. Her dermatologist recommended cessation of Maxitrol ophthalmic ointment and started hydrocortisone ointment for the periocular skin.
The patient followed up with her glaucoma specialist and her Cosopt (dorzolamide-timolol) drops were stopped. She was started on latanoprost for management of her intraocular pressure. Her periocular dermatitis resolved completely shortly after discontinuation of her Cosopt (dorzolamide-timolol) drops as shown in Figure 2.

Figure 2: External photograph demonstrating resolution of periocular rash.
Periocular dermatitis due to Cosopt (dorzolamide-timolol)
Periocular dermatitis is an inflammatory skin disorder producing an erythematous and pruritic rash involving the skin that surrounds the eye. It is important for clinicians to understand the etiology, broad differential diagnosis, and treatment strategy for this disease process. This dermatologic condition can be challenging for physicians to treat and emotionally stressful to experience as a patient.
Periocular dermatitis predominantly occurs in women over the age of 40 [1,2]. The increased prevalence of women with this disease may be associated with the use of various facial cosmetic products such as makeup, moisturizers, and perfumes [1,2]. The increased prevalence with age may be associated with the use of ocular medications (i.e. glaucoma drops), which are more common in older populations [3].
The exact etiology in each instance of this dermatologic condition is not always well understood but is likely the result of a complex interaction between genetic and environmental risk factors. The most common known causes of periocular dermatitis include allergic contact dermatitis, atopic dermatitis, airborne dermatitis, irritant contact dermatitis, rosacea, and psoriasis [1 ,2].
Patients with this condition typically present with a periocular rash that is pruritic or has a burning sensation. Clinical features of the rash include small erythematous papules or pustules overlying an erythematous and scaly patch of skin surrounding the eye, which may involve the upper and or lower eyelids. Surrounding skin edema is also common. The rash is usually localized but may also be associated with perioral dermatitis, or a rash surrounding the mouth and nose. It is often a clinical diagnosis and additional workup is usually not undertaken. If indicated, allergen testing with dermatology may be pursued. If a skin biopsy is performed, histological examination reveals non-specific inflammation with lymhpohistiocytic inflammation in a perifollicular or perivascular pattern [4]
The cornerstone of treatment is stopping the offending agent, which may include topical eye drops such as glaucoma medications, topical corticosteroids, skin moisturizers, sunscreen, and makeup. It is prudent to taper topical corticosteroids as immediate cessation may result in a more severe inflammatory response. Topical corticosteroids bind intracellular receptors to affect the nuclear factor kappa B pathway, which blocks the synthesis of inflammatory cytokines [for review, see 5]. For mild disease, topical calcineurin inhibitors such as tacrolimus are beneficial. Calcineurin inhibitors have been shown to be helpful and safe for inflammatory skin diseases involving the face and reduce inflammation by blocking T-cells from releasing pro-inflammatory cytokines [6]. For severe disease, oral antibiotics such as tetracyclines and macrolides as well as isotretinoin may be beneficial and oral therapy may be needed for several months.
In addition to medical therapy, providing emotional support for patients is also important. Periocular dermatitis can be stressful for patients as the rash is highly visible, involves the face, and may sometimes be persistent despite multiple therapies. Steroid-induced skin changes such as skin atrophy and telangiectasias contribute to distress.
EPIDEMIOLOGY OR ETIOLOGY
|
SIGNS
|
SYMPTOMS
|
TREATMENT/MANAGEMENT
|
Ong JE, Quist TS, Laageide L, Ko AC. Periocular Dermatitis and Cicatricial Ectropion Secondary to Cosopt (Dorzolamide-Timolol). EyeRounds.org. Posted October 30, 2019; Available from https://EyeRounds.org/cases/289-periocular-dermatitis.htm

Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.

Address
University of IowaLegal
Related Links
