

Optics and Refraction: From One Medical Student to Another
Authors: Logan Wolfel, BA; Christopher Fortenbach, MD, PhD; Caroline Yu, MD; Pavlina Kemp, MD
Posted May 20, 2021
Introduction
Over 150 million American adults utilize corrective lenses, such as glasses or contact lenses, every day. Without corrective lenses, millions of individuals would suffer from debilitating visual impairment [1]. While the causes of refractive error vary, they ultimately lead to an inability of the eye to focus light onto the retina.
In this article we will introduce optics of the normal eye and eyes with refractive error. We will also discuss treatment options for various refractive errors and describe how to interpret glasses and contact lens prescriptions.
Normal Eye Optics
Light is refracted by both the cornea and lens before reaching the retina. In order for a normal eye to produce a clear image, light rays are bent by the cornea and lens and focused on a single point of the retina, the fovea, designated as the focal point (Figure 1). This process is known as refraction, and the degree to which light is bent by a substance is measured in diopters [2,3]
A diopter is a unit of refractive power of a lens equal to the reciprocal of the focal length measured in meters (m-1). Converging lenses have a positive dioptric power, and diverging lenses have a negative dioptric power (Table 1).
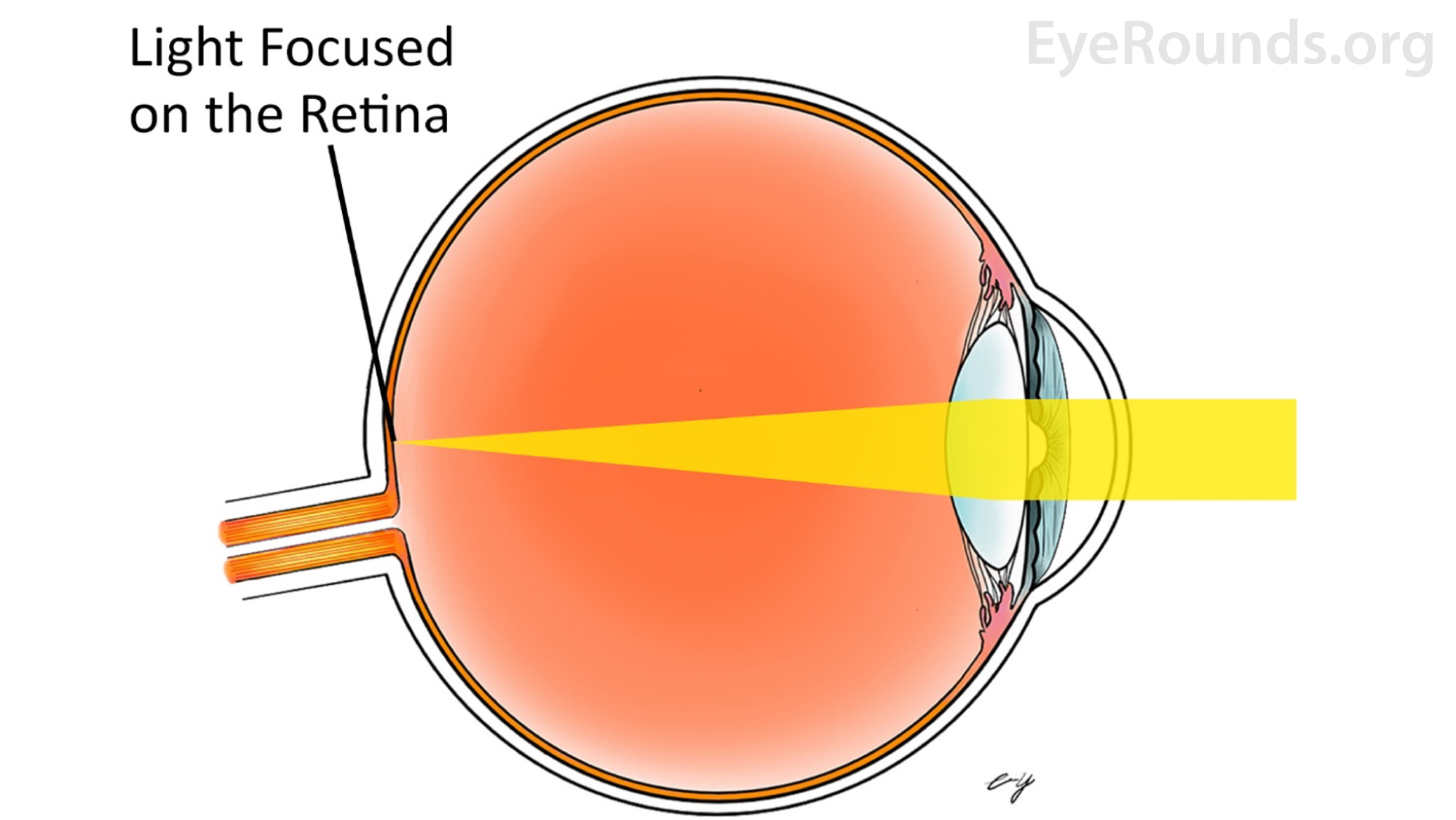
Figure 1: Representation of light refraction in the normal eye
Number of Diopters |
1/ Diopters (1/m) |
Focal Length |
1 |
1/1 |
1m =100cm |
2 |
1/2 |
0.50m =50cm |
3 |
1/3 |
0.333m =33.3cm |
4 |
1/4 |
0.25m =25cm |
5 |
1/5 |
0.20m =20cm |
6 |
1/6 |
0.166m =16.6cm |
8 |
1/8 |
0.125m =12.5cm |
10 |
1/10 |
0.10m =10cm |
Table 1: Relationship between diopters and focal length. Converging lenses have a positive dioptric power, where the focal point lies on the opposite side of the lens as the incident light. For example: a 2 diopter lens has a focal length of ![]() meters or 50cm, indicating a converging lens that focuses parallel incident light rays to a point 50cm from the lens. Diverging lenses have a negative power indicating that the focal point lies on the same side of the lens as the incident light. For a -3 diopter lens, the lens's focal point will be on the same side of the incident light at a distance of
meters or 50cm, indicating a converging lens that focuses parallel incident light rays to a point 50cm from the lens. Diverging lenses have a negative power indicating that the focal point lies on the same side of the lens as the incident light. For a -3 diopter lens, the lens's focal point will be on the same side of the incident light at a distance of ![]() of a meter or 33.3cm.
of a meter or 33.3cm.
Myopia
Myopia, also known as near-sightedness, causes a patient to see objects at near more clearly than objects at distance. The most common causes of myopia are increased axial eye length or excessive refractive power of the cornea or lens. In these scenarios, light is focused anterior to the retina resulting in a blurry image [4] (Figure 2).
As myopia causes light to focus anterior to the retina, correction is achieved with a diverging or concave lens. As light strikes a diverging lens, the focal point is shifted posteriorly on to the retina generating a clear image.
In addition to severe visual impairment, highly myopic patients (commonly defined as more than 5 diopters of myopia) are at increased risk for further eye pathologies including myopic macular degeneration and retinal detachment [4][5]. Further discussion on pathologic myopia can be found an another Eyerounds article.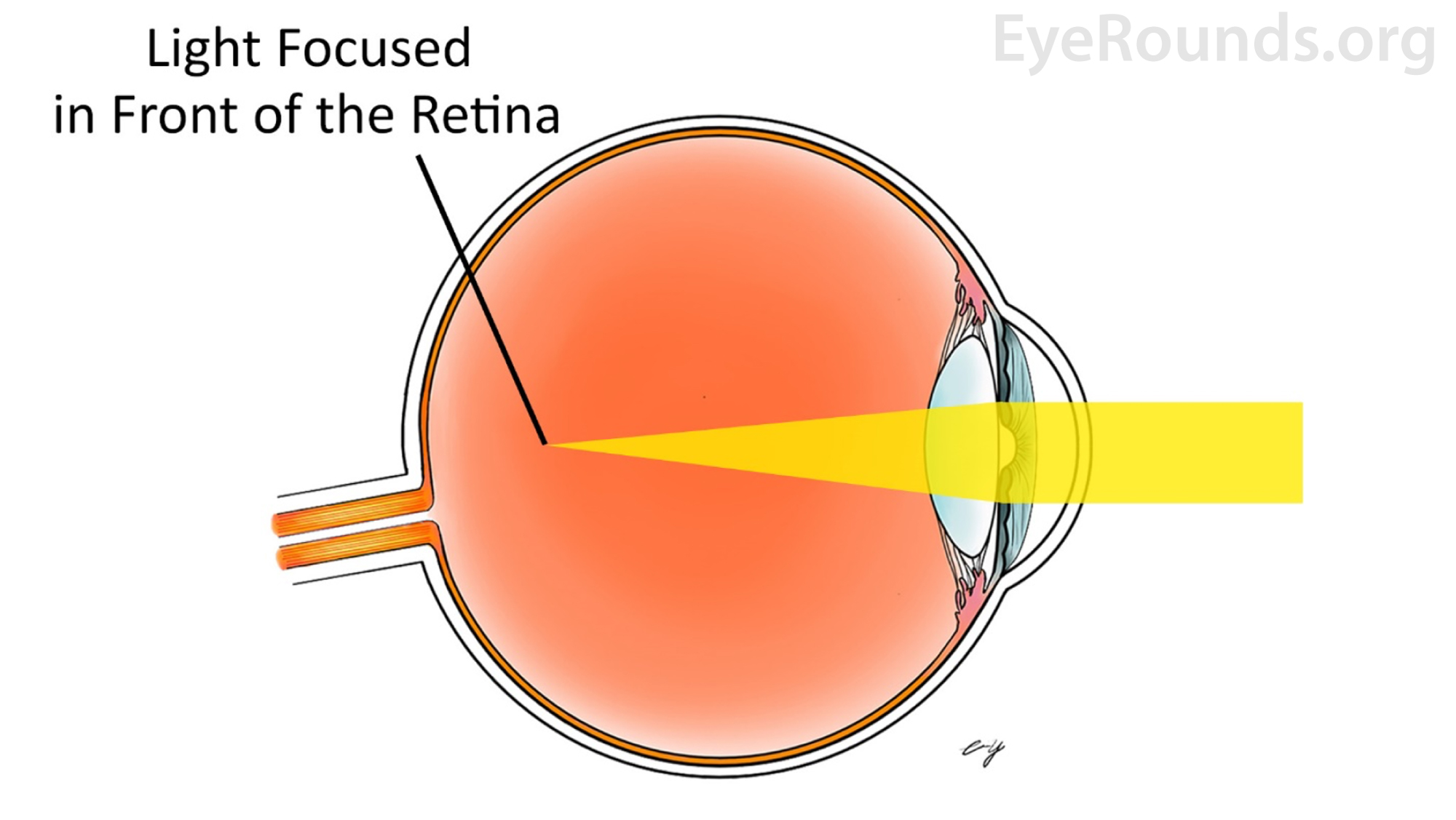
Figure 2: In myopia, the eye is too long or the cornea is too steep. Distant objects appear blurry because images are focused anterior to the retina.
Hyperopia
Hyperopia, also known as far sightedness causes patients to see objects more clearly at distance compared to near. Like myopia, hyperopia can stem from a variety of issues, including insufficient refractive power of the cornea or the lens, or a shortened axial eye length. These scenarios all result in light focused posterior to the retina [6] (Figure 3).
Correction of hyperopia is achieved with converging (convex) lenses. As light strikes a converging lens the focal point is displaced anteriorly onto the retina forming a clear image [6].
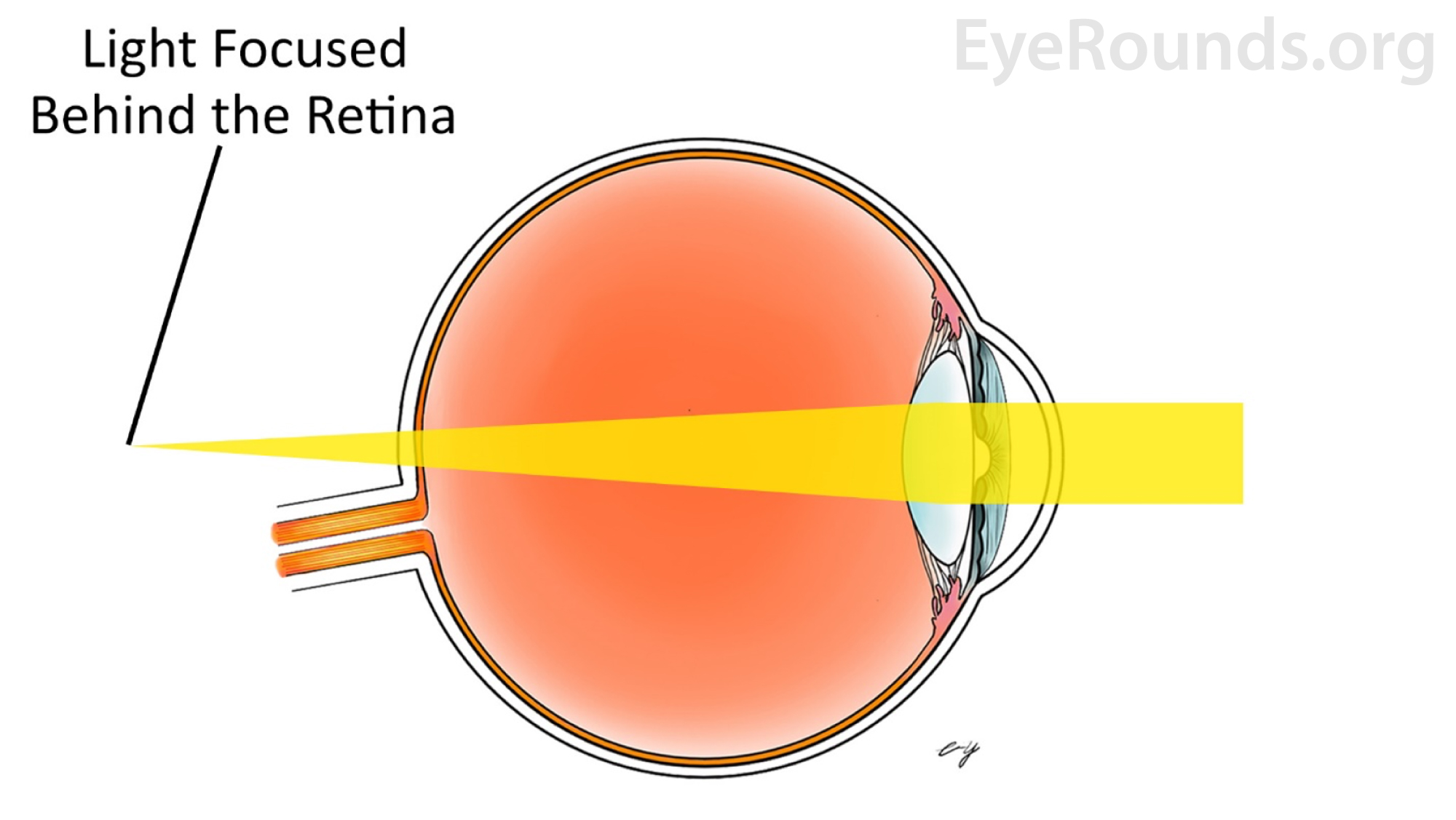
Figure 3: In hyperopia, the eye is too short or the cornea is too flat. As a generalization, close objects appear blurry because images are focused behind the retina.
Presbyopia
The human lens is composed of roughly 35% protein, which is the highest protein concentration of any tissue in the body. This affords the lens several unique properties including optical clarity and flexibility [7]. The lens is held in place by a series of bands known as zonules, which extend from the ring-shaped ciliary body and attach to the equator of the lens. The ciliary body muscle is ring-shaped, therefore contraction decreases the diameter of the ring and decreases zonular tension. This decreased tension allows the lens to become more spherical which increases the refractive index and improves near vision. This process is known as accommodation[8] (Figure 4).
During the natural aging process, the lens loses its elasticity and becomes fixed in a flatter configuration [8]. This impairs the ability to assume a spherical shape necessary for accommodation. This loss of accommodation is known as presbyopia and typically becomes clinically significant in the 5th decade of life. The loss of accommodation causes blurry vision when looking at near objects and hinders the ability to read books or electronics and perform any other activities that require near vision [9].
As presbyopia is an impairment of near vison, the treatment is to add lenses with positive power that converge light to compensate for diminished accommodation. When only correcting for near vision, these lenses are known as reading glasses and can be purchased at most pharmacies without the need for a prescription. Likewise, reading lenses can be added to traditional glasses to form bifocal lenses that have prescriptions for both near and distance vision. Additionally, in some cases trifocal or progressive lenses can be added to a patient's prescription to account for near, intermediate and distance vision [10] (Figure 5).
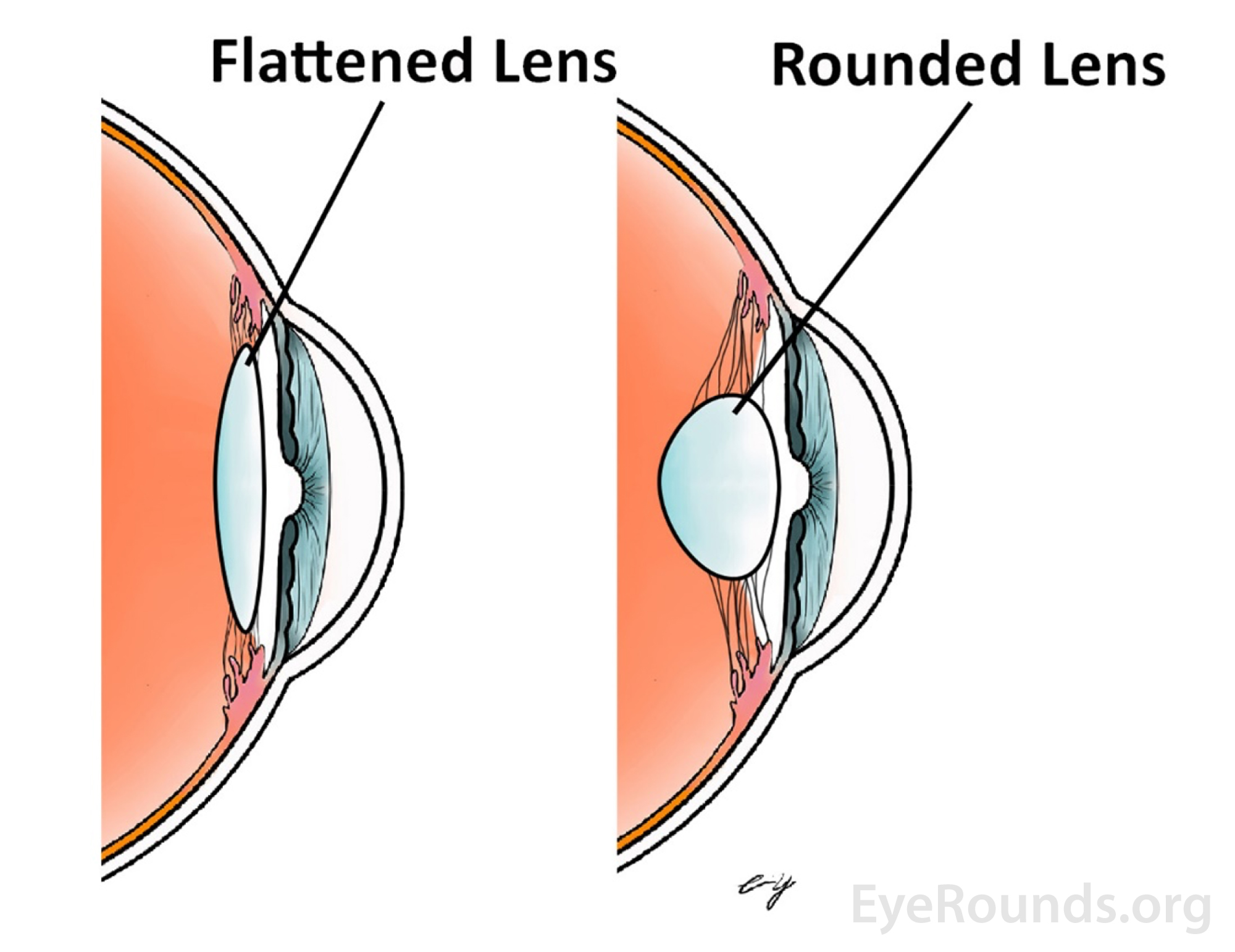
Figure 4: Shape of an accommodated lens (right) and a non-accommodated lens (left), exaggerated here to highlight the changes during accommodation.
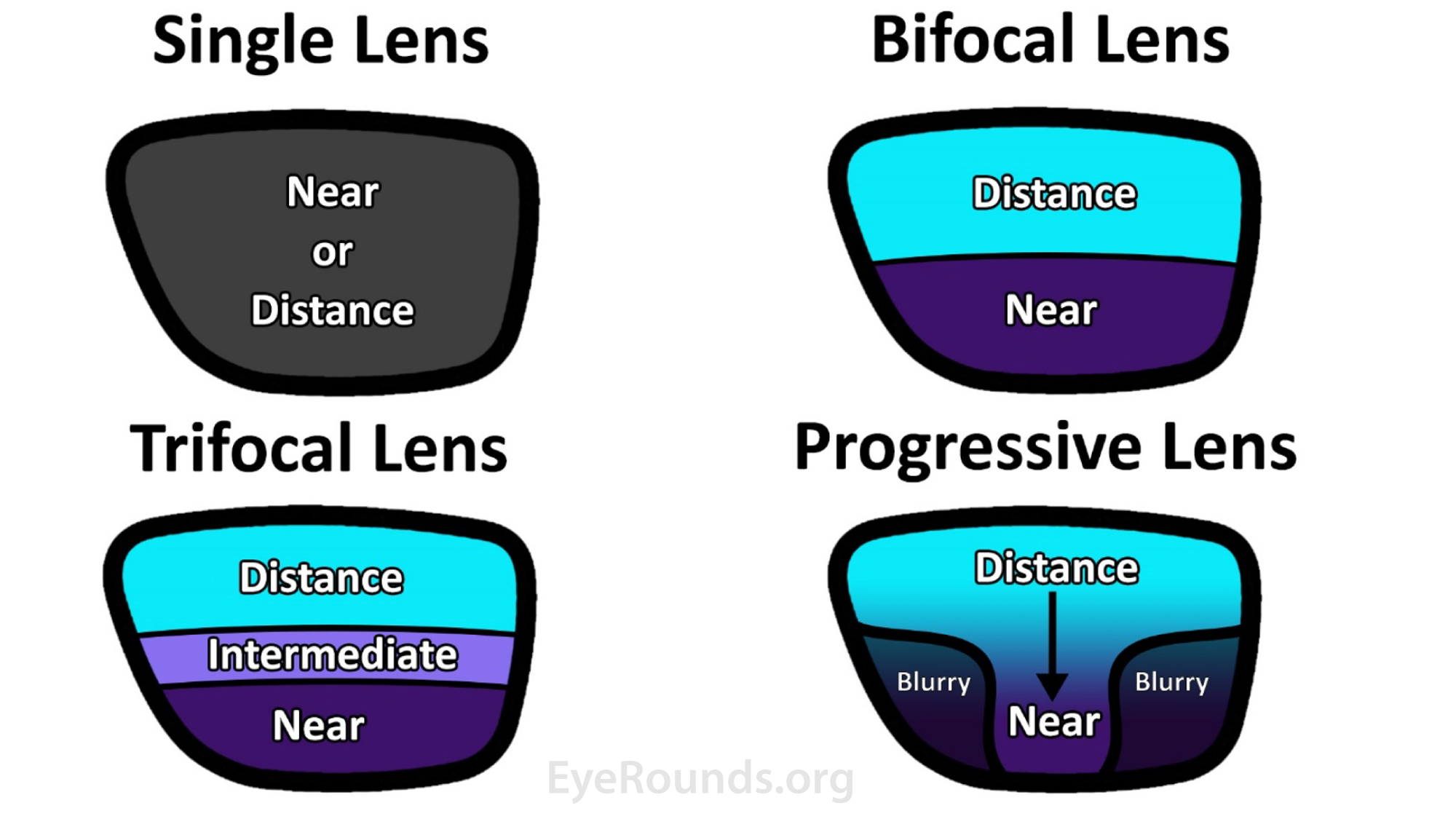
Figure 5: Corrective lens options for variable distances.
Astigmatism
The cornea is responsible for roughly two thirds, or 40 diopters, of the refractive power of the eye; refractive errors originating in the cornea can lead to visual abnormalities [3]. Astigmatism is defined as an imperfection in the curvature of the cornea. A normal eye has a spherical curvature, and an astigmatic eye has an unevenly shaped cornea that more closely resembles a football, more steeply curved in one axis than the other. This unevenness of the cornea prevents light rays from forming a singular focal point on the retina [11] (Figure 6), which results in blurring at all viewing distances and angled glare around lights [12].
Unlike myopia or hyperopia which are corrected with spherical lenses, regular astigmatism is corrected with cylindrical lenses. Instead of the singular focal point generated with spherical lenses, cylindrical lenses generate a focal plane. A cylindrical lens is oriented according to the astigmatic axis of deviation and counteracts the abnormal curvature of the cornea. Peak corneal steepness along the vertical (90 degree) meridian is known as with-the-rule astigmatism, which is the most common type of astigmatism, while peak steepness along the horizontal (180 degree) meridian is known as against-the-rule astigmatism.
In the event corneal astigmatism cannot be corrected with a cylindrical lens, it is referred to as irregular astigmatism which may be a result of corneal trauma, corneal ulceration, keratoconus, or several other defects.
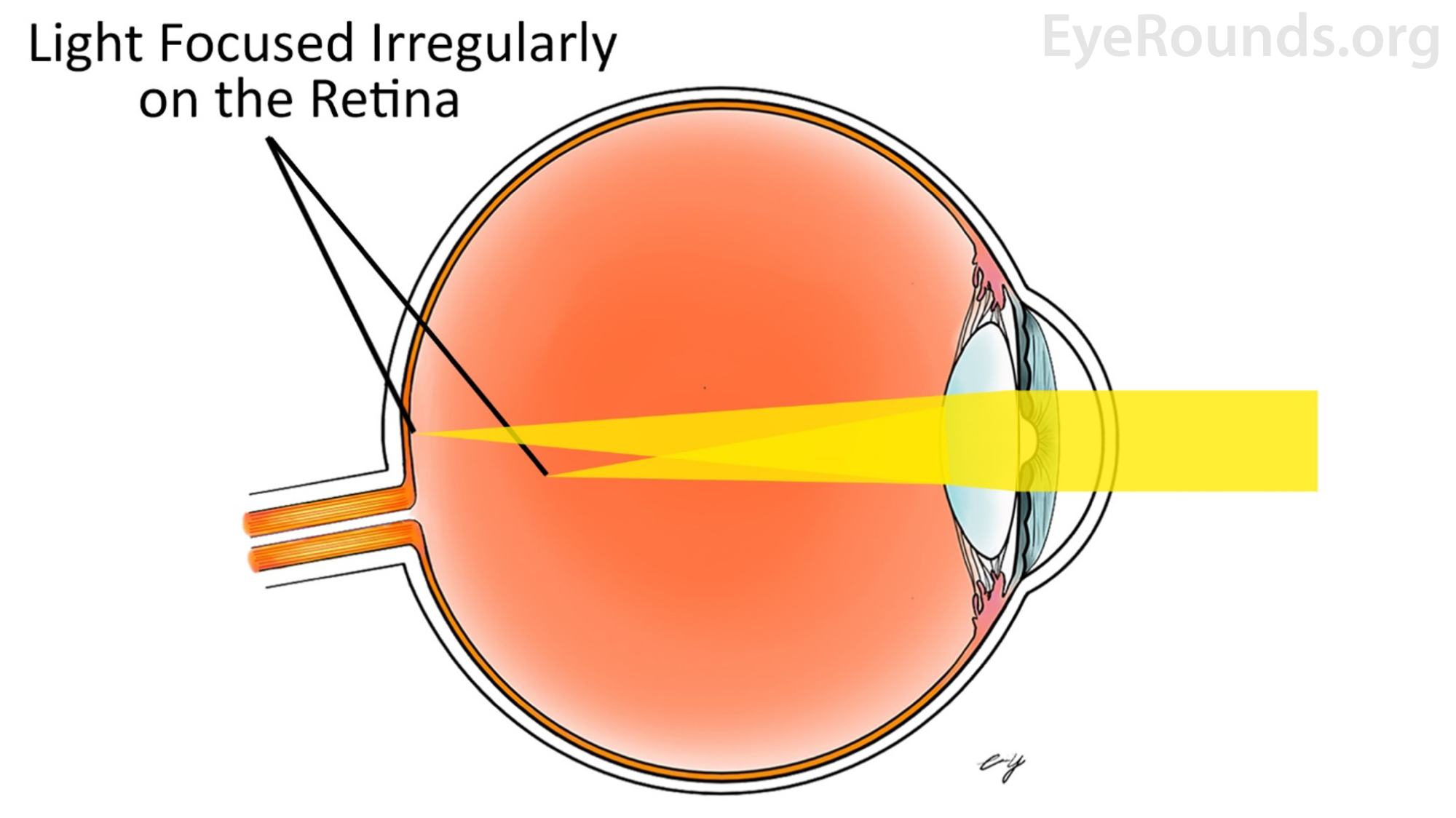
Figure 6: An astigmatic eye has an unevenly shaped cornea causing both close and distant objects to appear blurry.
How to Read a Glasses Prescription
Every year, millions of patients receive a prescription for glasses [1]. Interpretation of these prescriptions can be challenging due to numerous abbreviations and unfamiliar terminology.
The first step in deciphering a prescription is to recognize the abbreviations OD and OS, which stand for Oculus Dexter and Oculus Sinister, respectively. OD refers to the right eye and OS refers to the left eye. The abbreviation OU stands for Oculus Uterque and refers to both eyes [3].
Spherical correction (Sph) is represented by a positive (+) or negative (-) number, where the "+" indicates a converging lens which corrects hyperopia, and the "-" indicates a diverging lens which corrects myopia.
The next two values, Cyl and Axis, will only be listed if the patient requires astigmatic correction. Cyl is an abbreviation of cylindrical power which determines the strength of cylindrical lens needed to correct the astigmatism. As this is a cylindrical lens, it requires an orientation, therefore, an axis must also be reported [14], preferably with a three-digit number (i.e., axis at 90 degrees is reported "090").
Cyl can be reported in plus- or minus-notation, based on the convention of the prescriber. Optometrists often report cylinder power in minus notation, while ophthalmologists often report in plus cylinder power. To convert, or "transpose" one form of notation to the other, sum the Sph and Cyl (including positive and negative numbers), change the Cyl from plus to minus or minus to plus, and rotate the axis by 90 degrees (Figure 7). In the common event of a patient with both spherical and cylindrical refractive error, the final glasses prescription will contain spherocylindrical lenses. If there is no astigmatism, "Sph" is commonly written in the Cyl box, to indicate a complete prescription has been written.
|
SPH |
CYL |
Axis |
Minus Cylinder Notation |
+3.00 |
-2.00 |
060 |
Plus Cylinder Notation |
+1.00 |
+2.00 |
150 |
Figure 7: Example conversion from minus (-) cylinder notation to plus (+) cylinder notation.
The final values that can be included in an eyeglasses prescription (Figure 8) are Add, PD, and Prism. Add represents an additional spherical correction for reading with bifocal or progressive lenses. PD stands for Pupillary Distance, which is the distance in millimeters between the pupils. Prism is a specialized addition to lenses only for patients with diplopia or double vison. Prism aids in forming a single image, but further discussion is beyond the scope of this article [16].
|
SPH |
CYL |
AXIS |
PRISM |
ADD |
OD |
+2.00 |
-0.50 |
120 |
|
+2.25 |
OS |
+2.00 |
-0.50 |
120 |
|
+2.25 |
|
PD: 64 |
|
|||
Figure 8: A typical prescription for glasses include OD and OS values for Sph, Axis, Cyl, and under certain circumstances Add and Prism [17].
Glasses Prescription vs Contact Lens Prescription
Contact lens prescriptions share some of the same abbreviations used in prescriptions for glasses with a few key differences. When comparing a contact lens and glasses prescription, the Sph, Cyl, and Axis differ, as a contact lens sits directly on the surface of the eye, compared with approximately 12-14 mm away from the eye for glasses.
To ensure an appropriate fit, two additional values are included in a contact lens prescription. The first measurement necessary for contact prescriptions is the base curvature (BC). BC is a measurement of the total curvature of the contact lens that is adjusted to match the curvature of the patient's cornea. The next piece of additional information needed in a contact prescription is the diameter of the lens (Dia). This measurement is the distance from one edge of the contact lens to the other in millimeters. The final piece of information needed for a contact prescription is the brand of the contact lens. The brand is an essential component of a contact prescription because contact lenses with an identical prescription may fit differently (Figure 9).
|
SPH |
BC |
DIA |
AXIS |
CYL |
ADD |
Brand |
OD |
-1.50 |
8.6 |
14.5 |
160 |
-2.25 |
+1.00 |
- |
OS |
-1.50 |
8.6 |
14.5 |
160 |
-2.25 |
+1.00 |
- |
Figure 9: Similar to glasses, a typical prescription for contact lenses includes OD and OS values for Sph, Axis and Cyl, however it also includes values for BC, Dia, and the brand of contact prescribed [17].
References
- Vision Problems in the U.S.: Prevalence of Adult Vision Impairment and Age-Related Eye Disease in America. Prevent Blindness America and the National Eye Institute, 2008.
- Root, T. (2015). Chapter 9: Optics. In 932457446 730177716 T. Root (Author), OphthoBook (pp. 117-126). Tampa Bay, FL: Timothy Root.
- BRODIE, S. C. O. T. T. E. (2020). 2020-2021 Basic And Clinical Science Course (Bcsc), Section 03: clinical optics. AMER ACADEMY OF OPHTHALMOGY.
- Friedman NJ, Kaiser PK. Essentials of Ophthalmology. Philadelphia, PA: Elsevier Inc; 2007:253-254.
- Williams, K., & Hammond, C. (2019). High myopia and its risks. Community eye health, 32(105), 5–6.
- Moore BD, Augsburger AR, Ciner EB, Cockrell DA, Fern KD, Harb E. Optometric Clinical Practice Guideline: Care of the Patient with Hyperopia. St. Louis, MO: American Optometric Association; 1997:1-29
- Root, T. (2015). Chapter 2: Anatomy of the Eye. In 932457446 730177716 T. Root (Author), OphthoBook (pp. 21-32). Tampa Bay, FL: Timothy Root.
- American Optometric Association. Care of the patient with presbyopia. St. Louis (MO): American Optometric Association; 2010.
- Cavallotti, C., & Cerulli, L. (2010). Age-related changes of the human eye. Totowa, NJ: Humana Press.
- Boyd, Kierstan (January 12, 2020). "Presbyopia Treatment". American Academy of Ophthalmology. Retrieved 9-17-2020
- "Facts About Astigmatism". National Eye Institute. October 2010. Archived from the original on 2 October 2016. Retrieved 9-16-2020.
- Vimont, C. & Tubert, D. (August 31, 2018). "What do Astigmatism Measurements Mean?". American Academy of Ophthalmology. Retrieved 9-17-2020
- "Refreactive Errors". National Eye Institute. August 2020. Retrieved 9-17-2020.
- Vimont, C. & Tubert, D. (August 31, 2018). "What do Astigmatism Measurements Mean?". American Academy of Ophthalmology. Retrieved 9-17-2020
- Porter, Daniel (May 6, 2020). "Eyeglasses Prescription". American Academy of Ophthalmology. Retrieved 9-17-2020
- Michel Millodot (2014-07-30). Dictionary of Optometry and Visual Science E-Book. Elsevier Health Sciences. pp. 101
- Jürgens, I. (2019, June 17). How to understand an eyeglass prescription? - Institut Català de Retina. Retrieved September 17, 2020, from https://icrcat.com/en/how-to-understand-an-eyeglass-prescription/
Suggested Citation Format
Wolfel L, Fortenbach C, Yu C, Kemp P. Optics and Refraction: From One Medical Student to Another. EyeRounds.org. May 20, 2021. Available from https://EyeRounds.org/tutorials/optics-and-refractions-medical-student/index.htm