

Thyroid Eye Disease: An Introductory Tutorial and Overview of Disease
Clinical Presentation
The thyroid state of a patient presenting with TED is quite variable: 90% hyperthyroid, 6% euthyroid, 3% with Hashimoto's thyroiditis, and 1% hypothyroid [2]. Patients are simultaneously diagnosed with TED and thyroid dysfunction 20% of the time, and 60% present within 1 year of onset of thyroid disease [9]. However, TED can present long before (up to 10 years) or long after (up to 20 years) the initial presentation of thyroid disease [2].
TED is a self-limiting disease and may present in one of two stages: active or quiescent (Figure 6). In the active stage, there is active inflammation, which can lead to orbital muscle enlargement, conjunctival injection and chemosis, ocular pain, and swelling of the periocular tissues and eyelids. This stage typically involves waxing and waning TED symptoms and can last months to years. On average, the active phase lasts for 1 year in non-smokers and 2-3 years in smokers. The quiescent phase follows spontaneous resolution of the active phase (Figure 7). Active TED has a recurrence rate of 5-10% but is less likely to recur after 18 months of quiescence [10].

Figure 6: Active vs. Stable TED. Active TED is characterized by signs of inflammation (orbital muscle enlargement, conjunctival injection, swelling of periocular tissue, and chemosis). TED activity waxes and wanes, and usually transitions to stable TED within 1-3 years.

Figure 7: Rundle's curve. As seen in the representation of TED activity over time in Rundle's curve, early initiation of therapy is crucial in diminishing the final severity of disease manifestations.
- Upper eyelid retraction – the most common presenting sign of TED (Figure 8)
- Up to 90% of patients affected (bilateral or unilateral) [2]
- Multifactorial cause [2]
- Increased sympathetic tone acting on Müller's muscle
- Contraction of the levator palpebrae superioris
- Proptosis
- Scarring between the lacrimal gland and the levator palpebrae superioris
- Physical exam
- Dalrymple's sign (Figure 8): widening of the palpebral fissure with inferior and superior scleral show
- Lagophthalmos (Figure 9)
- Inability to close the eyes completely
- Manifests as dry eye, tearing, foreign body sensation, blurred vision, and eventually exposure keratopathy, especially with a poor Bell's reflex
- Temporal flare (Figure 10): elevation of the temporal upper eyelid compared to its normal anatomical location
- see Treatment options

Figure 8: Eyelid retraction is the most common presenting sign of TED, and is the result of many factors associated with TED. This image also shows Dalrymple's sign, characterized by the widening of the palpebral fissure. Note the superior and inferior scleral show.
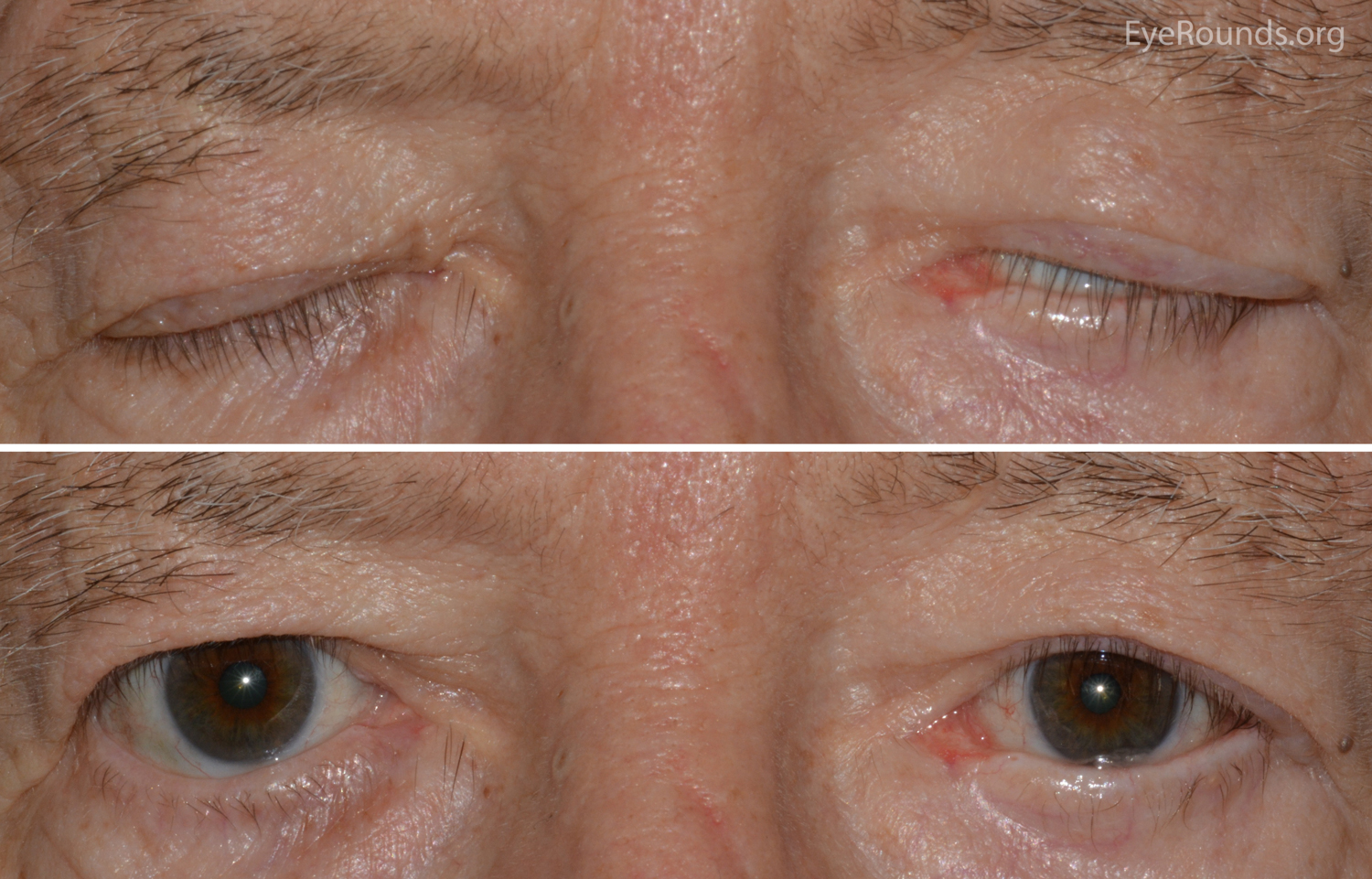
Figure 9: Lagophthalmos. Lagophthalmos typically presents as dry eye, tearing, foreign body sensation, and blurred vision.

Figure 10: Temporal flare. Note the elevation of the temporal portion of the upper eyelid.
- Exophthalmos – the second most common sign associated with TED (Figure 11)
- 60% of patients are affected [2]
- Physical exam
- Exposure keratopathy: characteristic punctate epithelial erosions
- Globe subluxation: anterior displacement of the globe [11]
- Globe equator protrudes anteriorly in relation to the lids
- Ophthalmologic emergency
- Decreased perfusion of the optic nerve and the retina
- Anoxic destruction of the optic nerve can cause irreversible visual loss
- see Treatment options

Figure 11: Exophthalmos. The globe is displaced anteriorly out of the orbit. This is an ophthalmologic emergency – the cornea is at risk for exposure, and the optic nerve is at risk of irreversible damage.
- Other common signs and symptoms associated with TED: eyelid lag, extraocular myopathy, pain with eye movement, optic neuropathy, chemosis, and conjunctival injection
- Eyelid lag
- 50% of patients affected
- Static dysfunction in which the upper eyelid is elevated in relation to the globe while in downgaze
- Von Graefe's sign
- Dynamic form of eyelid lag associated with TED
- Delayed descent of the upper eyelid during downgaze
- Restrictive extraocular myopathy (Figures 13 and 14)
- 40% of patients affected
- Inferior and medial rectus muscles most commonly affected, leading to hypotropia and esotropia, respectively
- Corneal light reflex –
- Clinical examination in which position of light reflex relative to pupil and limbus is used to evaluate degree of duction in the four cardinal directions
- Shown to be the best method of evaluating restrictive extraocular myopathy [12]

Figure 12: Hypotropia. Note the vertical misalignment of the eyes in primary gaze and the restrictive movement in upward gaze. This is due to an enlarged and restricted inferior rectus muscle.

Figure 13: Esotropia. Note the horizontal misalignment of the eyes in primary gaze. This is due to an enlarged and restricted medial rectus muscle.
- Pain with eye movement [2]
- 30% of patients affected
- Characterized as dull, deep orbital pain
- Optic nerve dysfunction from compressive optic neuropathy (Figure 14) [2]
- 6% of patients affected
- Compression of the optic nerve due to enlargement of the rectus muscles and increased volume of periorbital tissue within the confines of the bony orbit
- Presents with dyschromatopsia, decreased vision, and/or visual field defects
- Ophthalmic emergency requiring immediate treatment
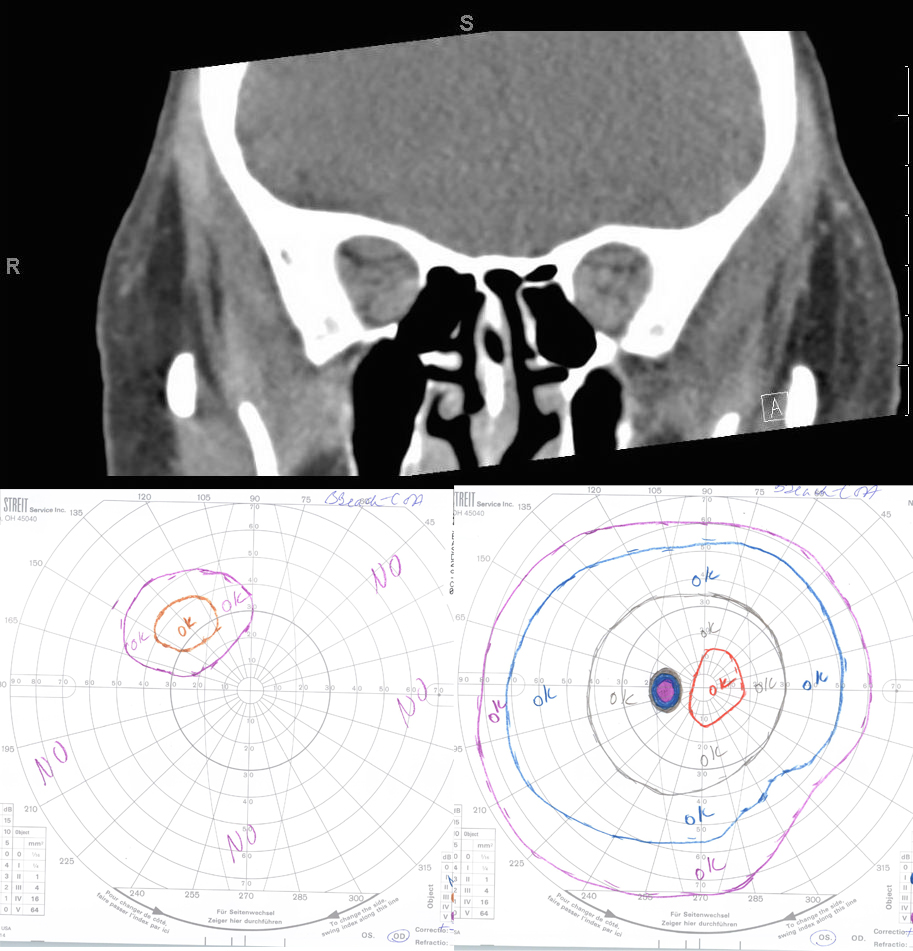

Figure 14: Compressive optic neuropathy. This sequence shows a series of CT scans from patients with compressive optic neuropathy, with their associated visual fields.
- Chemosis and conjunctival injection (Figures 15 and 16)
- Sign of active inflammation cause by congestion of the orbital tissue
- More pronounced at the site of the rectus muscle insertion

Figure 15: Chemosis. Note the swelling within the conjunctiva.

Figure 16: Conjunctival Injection. Note the dilation of the nasal and temporal conjunctival vessels. (larger image not available)
- Exposure keratopathy (Figure 17)
- Secondary sign due to lagophthalmos from eyelid retraction and/or exophthalmos
- Predisposes the cornea to bacterial infection (keratitis), which can lead to ulceration, endophthalmitis, and perforation
- Multimodal management
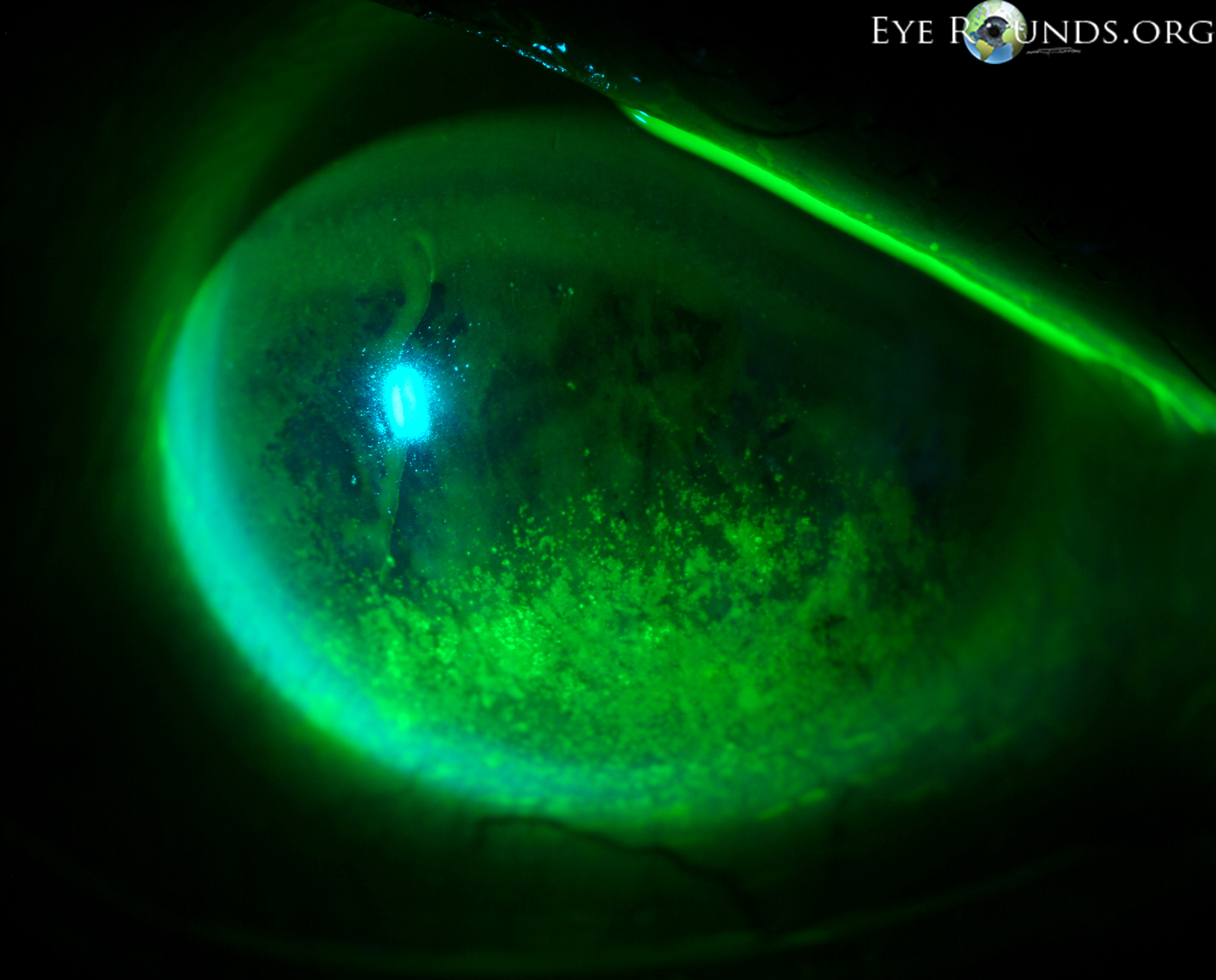
Figure 17: Exposure keratopathy. Punctate epithelial erosions (PEE) secondary to exposure keratopathy.